|
Comparing the Self-Esteem
and Resiliency between Blind and Sighted Children
and Adolescents in Kermanshah City
Saeedeh Bakhshi (1)
Nafiseh Montazeri (2)
Babak Nazari (3)
Arash Ziapour (4)
Hashem Barahooyi (5)
Fatemeh Dehghan (6)
(1) Department of Internal Medicine, School
of Medicine, Kermanshah University of Medical
Sciences, Kermanshah, Iran
(2) Department of Cardiology, School of Medicine,
Kermanshah University of Medical Sciences, Kermanshah,
Iran
(3) Department of Radiology, School of Medicine,
Kermanshah University of Medical Sciences, Kermanshah,
Iran
(4) Students Research Committee, Kermanshah
University of Medical Sciences, Kermanshah,
Iran
(5) Department of Counseling, Faculty of Social
Sciences and Education, Razi University, Kermanshah,
Iran
(6) Department of Nursing, Faculty of Nursing
and Midwifery, Kermanshah University of Medical
Sciences, Kermanshah, Iran
Correspondence:
Fatemeh Dehghan
Department of Nursing, Faculty of Nursing and
Midwifery, Kermanshah University of Medical
Sciences, Kermanshah, Iran
Email: fateme.dehghan1368@gmail.co
|
Abstract
Introduction:
The lack of independent moving by
the blind predicts a delay in the development
of daily and social life skills. The purpose
of this study was to compare self-esteem
and resilience between blind and sighted
children and adolescents in Kermanshah
City.
Methods:
The research was causal-comparative type
and the statistical population included
all blind people 8 to 16 years old from
both sexes (males and females) who lived
in Kermanshah City in 2016. The number
of these people according to Kermanshah
Welfare Center was reported as 70 people
of whom 60 (30 males and 30 females) were
selected through available sampling method.
A total of 60 blind people were matched
in terms of education, gender and age
with a non-blind group. The research tool
consisted of Rosenberg Self-Esteem Questionnaire
(1965) and Connor & Davidson Resilience
(2003). Data were analyzed using SPSS-19
application and multivariate variance
test.
Findings: The
results showed that there was no significant
difference between the two blind and sighted
groups in the resilience rate (P> 0.01)
but there was a significant level of difference
in self-esteem among blind and sighted
people (P <0.01).
Conclusion:
It seems that disability exists not only
in the body of people with disabilities,
but also in the attitudes of those individuals
and other individuals in different societies.
Key words:
Self-Esteem, Resiliency, Sighted,
Children and Adolescents
|
Eyesight disorder is a general term indicating
a disability to see and can be mild and modifiable,
such as myopia, and hyperopia, or be severe
and irreversible, such as blindness or severe
eyesight impairment. Blindness may be congenital,
such as congenital cataract, congenital syphilis,
mother contracting rubella in during pregnancy
or it may be adventitious such as trachoma,
retinal detachment, eyesight acuity atrophy,
corneal ulcers, vitamin A deficiency, accident
or a shock and etc. Considering that the visual
forms almost a third of the total network fiber
of the human sense communication network and
this is not the case in any other senses, therefore
man should be described as an intuitive being.
For this reason, visual impairment causes disability
more than any other disability (1). The occurence
of blindness in infancy is 8 in 10,000 up to
the age of fourteen and with increasing age,
this ratio increases. At the age of 60, it reaches
to 44 per thousand (2). To Smith, self-esteem
is a person’ evaluation of themself or
specific judgments about their value. For those
with injury to their eyesight, adequacy and
appropriate social skill is a key factor for
self-positive, higher self-esteem, positive
behaviors and the ability to accept disability
as a part of their life. Self-esteem is the
judgment about our values and feelings associated
with these judgments (3).Self-esteem is a psychological
phenomenon that has a decisive influence on
human emotional and cognitive dimensions and
is a strong predictor of satisfaction with life.
Low self-esteem is a dangerous factor for negative
outcomes throughout life (4). Social isolation,
and lack of adequate social support among adolescents
with eyesight impairment may result in low self-esteem
(5).
Self-esteem is the judgment that a person has
about their own value. Self-esteem is considered
as a central and essential factor in the individuals’
emotional and social compatibility. A person
with high self-esteem has an appropriate attitude
towards themself and others; vice versa, a person
with low self-esteem is often isolated or in
desperation trying to show others and themselves
that they are deserving. Many emotional and
mental disorders in adolescents can be prevented
by providing mental health services and enhancing
self-esteem (6).
Increasing self-esteem is one of the most valuable
resources that people with eyesight impairment
can have. Studies have shown that people with
high self-esteem and eyesight disorder experience
much more effective learning and more useful
relationships and use opportunities better(7).
The lack of independent movement by the blind
predicts a delay in the development of daily
and social life skills (8). Considering that
emotional and social skills are learned in relation
to others and it is necessary to have the power
of sight for learning many of these skills,
as a result, blind people are deprived of such
experiences due to their eyesight impairment;
these experiences can have an impact on their
emotional excellence and social interaction(9).
Another psychology variable is resiliency which
applies to those who are in danger but do not
suffer from disturbances. Hence, it may be concluded
that exposure to risk is a necessary condition
for vulnerability but it is not sufficient.
Resiliency factors cause a person to uses his
or her existing capacity to achieve success
and growth in the face of risk factors and use
these challenges and quizzes as an opportunity
to empower himself (10, 11).
There are two common components in most resiliency
definitions: a) The individual responds positively
to the unpleasant situation and b) In this way,
the individual feels more self-confidence and
growth (12).
Waller (13) considers resiliency as a positive
person’s response to difficult conditions
(injuries and threats). Resiliency, of course,
is not just stability against injuries with
threatening conditions and is not a passive
state in dealing with dangerous conditions,
but it is an active and constructive accompaniment
in its perimeter environment. It can be said
that resiliency is the individual’s ability
to establish a biological-psychological balance
in a dangerous situation (14).
In physiology and medicine, resiliency represents
the self-efficacious physical resilience and
the ability to regain emotional balance in stressful
situations (15, 16).
In research done by Papadopoulos (9), the impact
of individual characteristics (gender, eyesight
status, age), age at eyesight loss, level of
education, employment status and ability to
move independently (without the need for help)
were studied on the source of control and adolescent
self-esteem with eyesight problems. The results
of this study showed that predictors of self-esteem
are eyesight status, age of the individual at
the time of eyesight loss and education level.
Gilmour (17)showed that wisdom, hope, and self-efficacy
can be predictors of resiliency in American-African
students. Papadopoulos et al.(18)compared the
source of control and self-esteem in adults
with eyesight impairment and in non-blind adults.
108 adults with eyesight impairment (blindness
or low eyesight) and 55 sighted adults participated
in this study. Sighted adults showed higher
scores in self-esteem than blind people with
low eyesight. The results did not show a significant
difference in the control scores of three groups.
In this study, the eyesight and age of a person
were determined at the time of loss of eyesight
as self-esteem predictors.
Mishra and Singh (19) conducted research aimed
at comparing the self-concept and the confidence
in children with eyesight impairment and sighted
children. The results of this study showed that
children with eyesight impairment have lower
self-concept and self-esteem compared to sighted
children but this difference was not significant
between boys and girls. Sanicar and Groom (20)
conducted research aimed at studying self-concept,
self-esteem and social support for those with
special needs. The results showed that the place
of study (education in ordinary schools and
schools for particular children) and the type
of disability impact on self-concept, self-esteem
and social support. There was also a significant
relationship between their self-concept and
social support.
Stewart and Yuen (21) examined the psychological
factors affecting resiliency in patients with
physical disorders. The results of this study
showed that psychological factors effect on
the resiliency, self-efficacy, self-esteem,
internal control source, optimism, psychological
hardiness, hope, self-empowerment, and acceptance
of the disease. Coping strategies such as positive
cognitive assessment, spirituality and active
coping also had a significant relationship with
resiliency.
Finger et al. (22) in a study reported that
people with eyesight impairment in terms of
movement, emotional state and constraint of
social activities have a lower quality of life
than healthy people. Bowen (23) conducted a
study to assess the levels of self-esteem among
60 children with eyesight impairment. The results
of this study showed that 70% of children had
high or normal levels of self-esteem. Girls
also showed higher levels of self-esteem than
boys.
Considering what was presented, there has not
been any published research in Iran about the
simultaneous comparison of the sum of self-esteem
and the resiliency variables between the blind
and the sighted. The present research is going
to answer the following questions: Is there
any significant difference between the blind
and sighted people in two self-esteem and resiliency
variables?
The research is an applied study in terms
of purpose, a causal-comparative (post-event)
type one and descriptive in terms of method.
The statistical population of this study included
all male and female children and adolescents
who were between the ages of 6 to 16 years old
from both sexes in Kermanshah City in the year
2014. The number of these people according to
Kermanshah’s well-being report was 70 of
whom 60 were selected by available sampling
method (30 male and 30 female). A total of 60
individuals were matched with the sighted group
in terms of education, gender and age. They
were then compared in two independent groups.
After completing the questionnaires, the responses
were encoded and collected data was extracted
and analyzed according to the goals and research
questionnaire by self-esteem and resiliency
statistical tests.
|
ROSENBERG'S SELF-ESTEEM SCALE |
Rosenberg Self-Esteem Scale was prepared by the
Astronomical Day in 1965 to measure individuals’
self-esteem. The scale has 10 sections which were
classified from 1 to 4 and the respondent must
mark them in relation to the sensation in front
of each item. The validity coefficient of this
test was 0.3 in a study performed on a sample
of 82 subjects. This test has a good content due
to designing by Rosenberg to detect self-esteem
level. In addition, Rosenberg has calculated its
statistical indices during the process of setting
the test and has considered it to have validity.
In this study, Cronbach’s alpha reliability
coefficient was 0. 93 in a study done on female
students and in the test-retest reliability, r
= 0.85. Hart (24), believes that after the teenage
period, collective self-esteem is important. This
scale has been standardized in the sample of Iranian
teenagers and the reliability coefficient is 0.
84 (25). In this study, the reliability of the
research was obtained as 71% by Cronbach’s
alpha.
|
CONNER-DAVIDSON RESILIEANCE SCALE INVENTORY
(CD-RISC) |
The resiliency questionnaire was written by
Conner and Davidson (14) to measure the power
of coping with pressure and threat and Mohammadi
(26) has adapted it for use in Iran. The questionnaire
has 25 questions that are answered in five degrees
(perfectly correct, rarely correct, sometimes
correct, often correct and always correct) by
each subject. The validity coefficient of inner
consistency has been reported in the range of
0.86 to 0.90 using the Cronbach’s alpha
coefficient. The retest validity coefficient
of this scale was 0.81.
Mohammadi (26) has adapted this scale for use
in Iran. Soltani et al. (27) have obtained 0.87
the Cronbach Alpha coefficient of this scale
at students. In this study, the reliability
of the research obtained was 79% by Cronbach’s
alpha.
According to the research hypotheses, in the
present study, SPSS-23 application and variance
analysis test were used to realize the analysis
goals of the research in two descriptive and
inferential statistic parts.
Table 1: Frequency distribution and percentage
of sample examined based on gender
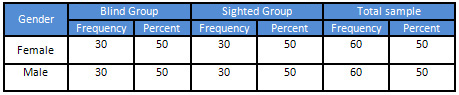
According to Table 1, the sample consisted of
120 people (60 sighted and 60 blind); every
blind and blind group consisted of 30 men and
30 women. Frequency distribution and sample
percent are in (Table 1) based on gender.
Table 2. Mean and standard deviation of
variables studied in two groups
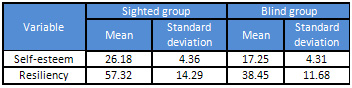
Table 3. The results of multivariate intergroup
variances analysis for analyzing the mean of
dependent variables
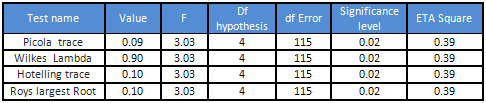
As shown in Table 3, the main effects of variance
analysis are significant and this means that
at least one of the dependent variables in two
groups has a significant difference. Therefore,
the intergroup variance analysis was used for
analyzing every variable. The results of the
intergroup variance analysis are presented in
(Table 4).
Table 4. An intergroup variance analysis
for measuring the difference of mean in two
groups

The results of variance analysis show that there
is a significant difference in resiliency and
self-esteem level (F = 8.98) in both groups.
The
main
purpose
of
this
research
was
to
compare
self-esteem
and
resiliency
between
blind
and
sighted
children
and
teenagers
in
Kermanshah
City.
As
Table
4
shows,
there
is
a
significant
difference
between
the
two
blind
and
sighted
groups’
self-esteem
and
comparing
the
means,
it
can
be
said
that
the
self-esteem
of
the
sighted
is
more
than
the
blind.
The
results
of
this
hypothesis
are
consistent
with
the
research
done
by
Beaty
(28),
Wolf
and
Sachs
(29),
Rosenblum(30),
Wagner
(5),
Lopez
and
Cordoba
(31),
Mishra
and
Singh
(19)
but
it
is
not
consistent
with
the
research
of
Mishra,
and
Singh.
(19).
It
seems
that
disability
exists
not
only
in
the
body
of
people
with
disabilities,
but
also
in
the
attitudes
of
those
individuals
and
other
individuals
in
different
societies.
These
negative
attitudes
and
psychosocial
obstacles
have
affected
the
mental
health
of
people
with
disabilities
and
made
them
have
lower
self-esteem
than
others.
The
inability
of
independent
movement
by
blind
people
in
Isfahan
was
a
predictor
of
the
delay
in
the
development
of
their
daily
and
social
life
skills.
Given
that
social
skills
are
learned
in
relation
to
others
and
it
is
needed
to
have
the
power
of
eyesight
for
many
of
these
skills,
as
a
result,
blind
people
were
deprived
of
such
experiences
due
to
their
eyesight
impairment.
These
experiences
could
have
had
an
impact
on
individuals’
self-esteem.
Social
isolation
and
the
lack
of
adequate
social
support
among
these
people
and
lack
of
special
facilities
for
training
in
their
jobs,
delayed
marriage
of
the
blinded
girls
in
Isfahan
and
the
negative
attitudes
of
society
towards
their
ability
cause
them
to
have
low
self-esteem.
Having
a
strong
sense
of
self-esteem
is
essential
for
all
people,
especially
children
and
adolescents
with
special
needs.
Self-esteem
as
a
valuable
vital
asset
is
one
of
the
most
important
factors
for
the
development
of
talent
and
creativity.
People
with
eyesight
impairment
or
other
disabilities
such
as
the
cause
of
parents’
negative
attitudes,
negative
experiences
in
dealing
with
ordinary
peers
and
successive
failure
at
school
and
college
are
gradually
discouraged
and
overwhelmed;
the
sequence
of
such
failures
and
problems
makes
them
feel
worthless,
a
sense
that
can
damage
their
self-esteem.
As
Table
4
shows,
there
is
a
significant
difference
between
the
resilience
of
blind
and
sighted
people
in
Isfahan
city.
The
results
of
this
hypothesis
are
consistent
with
the
research
of
Alrickson
et
al.
(32),
Zatra
et
al.
(33),
Nariman
et
al.
(34).
Some
scholars
believe
that
resilience
is
non-native
and
it
can
be
learned.
Resilience
is
affected
by
the
family.
Family
members
can
not
only
increase
social
ability
and
positive
self-esteem
but
they
can
also
increase
their
resilience
by
increasing
feedback
and
reinforcement
and
providing
more
interactive
opportunities
for
blind
people.
Family
support,
appropriate
feedback,
and
more
interaction
in
the
family,
make
them
more
immune
to
the
negative
effects
of
life
events
and
thus
reduce
their
risk
of
physical
and
mental
illness.
This
study,
like
any
other
research,
was
confronted
with
some
limitations
including:
Participants
in
this
research
were
blind
and
sighted
people
in
Isfahan
city.
Therefore,
caution
should
be
exercised
in
generalizing
the
results.
Another
limitation
is
the
low
volume
of
samples
that
may
affect
the
analysis
of
results
and
comparisons.
In
this
research,
available
sampling
method
was
used.
Therefore,
it
is
suggested
that
this
research
be
carried
out
in
a
wider
community
with
more
samples
in
other
cities
of
the
country,
other
psychological
variables
be
compared
among
blind
and
sighted
people,
and
in
future
research,
other
measurement
methods
(such
as
interviews)
should
be
used
to
provide
more
accurate
results.
1.
Milanifar
B.
Psychology
of
exceptional
children
and
adolescents.
Tehran:
Ghomes
Publication.
2007.
2.
Thylefors
B,
Negrel
A,
Pararajasegaram
R,
Dadzie
K.
Global
data
on
blindness.
Bulletin
of
the
world
health
organization.
1995;73(1):115.
3.
Peterson
CC.
Looking
forward
through
the
lifespan:
developmental
psychology:
Pearson
Higher
Education
AU;
2013.
4.
Erol
RY,
Orth
U.
Self-esteem
development
from
age
14
to
30
years:
a
longitudinal
study.
Journal
of
personality
and
social
psychology.
2011;101(3):607-19.
5.
Wagner
E.
Developmental
and
Implementation
of
a
curriculum
to
Develop
social
competence
For
student
with
visual
impairment
in
Germany.
Journal
of
Visual
Impairment
&
Blindness.
2004;98(11):703-10.
6.
Akolechy
M,
Mehri
A.
Assessment
of
Self
Esteem
among
Students
of
High
Schools
in
Sabzevar
(2010).
Tolooe
Behdasht.
2012;2(28-33).
7.
Goldestein
H,
Morgan
L.
social
interaction
and
modeles
of
friendship
development.
Available
site
:
http/wwwericcom.
2004.
8.
Dehghani
M,
Nazari
M.
The
comparison
of
Emotional
Quotient
in
blinds
and
low
visions
with
normal
sighted
people
in
Shahroud
welfare
organization,
1392.
Tehran:
Ghomes
Publication.
2014;1(1):32-41.
9.
Papadopoulos
K.
The
impact
of
individual
characteristics
in
self-esteem
and
locus
of
control
of
young
adults
with
visual
impairments.
Research
in
developmental
disabilities.
2014;35(3):671-5.
10.
Zarrinkelk
H.
The
effectiveness
of
training
aspects
of
resiliency
on
reducing
addiction
acceptance
and
changing
attitudes
toward
drug
use
among
high
school
students
in
Tehran:
MA
thesis.
AllameTabatabayi
University.
2010;
2010.
11.
Nazari
B,
Bakhshi
S,
Kaboudi
M,
Dehghan
F,
Ziapour
A,
Montazeri
N.
A
Comparison
of
Quality
of
Life,
Anxiety
and
Depression
in
Children
with
Cancer
and
Healthy
Children,
Kermanshah-Iran.
International
Journal
of
Pediatrics.
2017;5(7):5305-14
DOI:
10.22038/ijp.2017.3540.1978.
12.
Simon
JB,
Murphy
JJ,
Smith
SM.
Understanding
and
fostering
family
resilience.
The
Family
Journal.
2005;13(4):427-36.
13.
Waller
MA.
Resilience
in
ecosystemic
context:
Evolution
of
the
concept.
American
Journal
of
Orthopsychiatry.
2001;71(3):290-7.
14.
Connor
KM,
Davidson
JR.
Development
of
a
new
resilience
scale:
The
Connor-Davidson
resilience
scale
(CD-RISC).
Depression
and
anxiety.
2003;18(2):76-82.
15.
Shafiezadeh
R.
The
relationship
between
resilience
and
the
big
five
personality
factors.
Journal
of
knowledge
and
research
in
applied
psychology.
2012;13(1):95-102.
16.
Mohammadi
M,
Esfandnia
A,
Rezaei
S,
Ziapour
A.
Performance
evaluation
of
hospitals
under
supervision
of
kermanshah
medical
sciences
using
Pabon
Lasso
diagram
of
a
five-year
period
(2008-2012).
Life
Science
Journal.
2014;11
(1):77-81.
17.
Gilmore
AL.
A
Cultural
Examination
of
Hardiness:
Associations
with
Self-Esteem,
Wisdom,
Hope,
and
Coping-Efficacy.
2014.
18.
Papadopoulos
K,
Montgomery
AJ,
Chronopoulou
E.
The
impact
of
visual
impairments
in
self-esteem
and
locus
of
control.
Research
in
developmental
disabilities.
2013;34(12):4565-70.
19.
Mishra
V,
Singh
A.
A
comparative
study
of
self-concept
and
self-confidence
of
sighted
and
visually
impaired
children.
EXCEL
International
Journal
of
Multidisciplinary
Management
Studies.
2012;2(2):148-57.
20.
Seniar
M,
Kobal
Grum
D.
Self-concept
and
social
support
among
adolescents
with
disabilities
attending
special
and
mainstream
schools.
Hrvatska
revija
za
rehabilitacijska
istraživanja.
2012;48(1):73-83.
21.
Stewart
DE,
Yuen
T.
A
systematic
review
of
resilience
in
the
physically
ill.
Psychosomatics.
2011;52(3):199-209.
22.
Finger
RP,
Kupitz
DG,
Holz
FG,
Balasubramaniam
B,
Ramani
RV,
Lamoureux
EL,
et
al.
The
impact
of
the
severity
of
vision
loss
on
vision-related
quality
of
life
in
India:
an
evaluation
of
the
IND-VFQ-33.
Investigative
ophthalmology
&
visual
science.
2011;52(9):6081-8.
23.
Bowen
J.
Visual
impairment
and
its
impact
on
self-esteem.
British
Journal
of
Visual
Impairment.
2010;28(1):47-56.
24.
Harter
S.
Causes
and
consequences
of
low
self-esteem
in
children
and
adolescents.
Self-esteem:
Springer;
1993.
p.
87-116.
25.
Rajabi
G,
Bohlol
N.
Validity
and
Reliability
of
Rosenberg
Self-Esteem
Scale
in
First
Year
Student
of
Shahid
Chamran
University.
New
Educational
Approaches.
2006;3(2):33-48.
26.
Mohammadi
M,
Jazayeri
A,
Rafiie
&
Jokar
B,
Pourshahbaz
A.
Studying
the
effective
resiliency
factors
in
people
at
risk
of
drug
overuse.
psychology
scientific-
research
Journal,
University
of
Tabriz.
2005;3:193-214.
27.
Soltani
E,
Shareh
H,
Bahrainian
SA,
Farmani
A.
The
mediating
role
of
cognitive
flexibility
in
correlation
of
coping
styles
and
resilience
with
depression.
Pajoohandeh
Journal.
2013;18(2):88-96.
28.
Beaty
LA.
The
effects
of
visual
impairment
on
adolescents’
self-concept.
Journal
of
Visual
Impairment
&
Blindness.
1991.
29.
Wolffe
K,
Sacks
S.
The
Lifestyles
of
Blind,
Low
Vision,
and
Sighted
Youths:
A
Quantitative
Comparison.
Journal
of
Visual
Impairment
&
Blindness.
1997;91(3):245-57.
30.
Rosenblum
LP.
Perceptions
of
the
impact
of
visual
impairment
on
the
lives
of
adolescents.
Journal
of
Visual
Impairment
&
Blindness
(JVIB).
2000;94(07):434-47.
31.
López-Justicia
MD,
Córdoba
IN.
The
self-concept
of
spanish
young
adults
with
retinitis
pigmentosa.
Journal
of
Visual
Impairment
&
Blindness.
2006;100(6):366-400.
32.
Alriksson-Schmidt
AI,
Wallander
J,
Biasini
F.
Quality
of
life
and
resilience
in
adolescents
with
a
mobility
disability.
Journal
of
pediatric
psychology.
2006;32(3):370-9.
33.
Zautra
A,
Johnson
L,
Davis
M.
Runing
head:
Positveafect
enhances
resilencepositveafect
as
asource
of
resilence
for
women
in
chronic
pain.
Journal
of
Consulting
and
Clinical
Psychology.
2003;73(2):212-20.
34.
Narimani
M,
Talebi
Joibari
M,
Abolghasemi
A.
Comparison
of
documentary
style
and
resilience
among
students
who
are
injured
and
normal.
Psychology
of
Exceptional
Individuals.3(10):45-59.
|

