|
Treatment
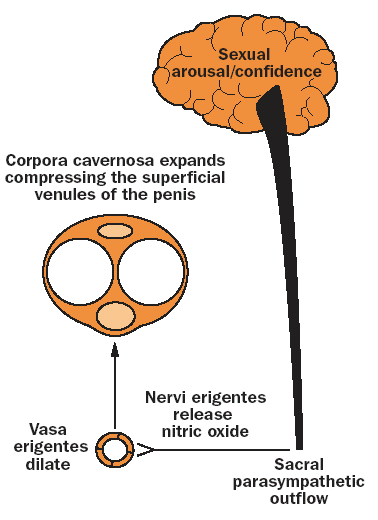
For an appreciation of the treatment of ED, an understanding of the physiology of erectile function
is very useful (Figure 1). The basic requirement for normal erectile function is the ability of the smooth
muscle of the corpus cavernosum to relax. During sexual arousal, this is mediated through the release
of nitric oxide (NO) from the para-sympathetic nerves, endothelial cells and possibly the corporeal
smooth muscle cells. The release of NO in the smooth muscle cells of the corporea leads to
relaxation of these cells mediated through c-GMP which is then converted by the enzyme PDE5 to
GMP. In the flaccid state arterial blood flow and
venous outflow are in equilibrium. The emissary veins are open and the cavernosal sinusoids and
arterioles are in a contracted state. Relaxation of the corporeal smooth cells expands the sinusoids
which become engorged with blood which itself becomes trapped as the emissary veins are themselves
compressed against the relatively unyielding tunica albuginea. Therefore, the penis is in an erect
state. For normal erectile function at the micro level, there needs to be, in order:
1. neural control (parasympathetics)
2. sinusoidal relaxation of the corpus cavernosa
3. arterial inflow to corpus cavernosa
4. venous occlusion from corpus cavernosum.
First line treatments
PDE5 inhibitors
The commonest cause of ED is insufficient sinusoidal relaxation (step 2 above). PDE5 inhibitors
(sildenafil, tadalafil), cause a 'build up' of c-GMP in the presence of sexual stimulation. It is important
to appreciate that PDE5 inhibitors' ability to treat ED is dependent upon the level of sexual arousal
(leading ultimately to release of NO) and thus cannot function as 'aphrodisiacs'. This is a common
misconception in the lay community leading to misuse or abuse of the medication. It may also lead
to a man being denied treatment by his partner who may feel offended that he needs such medications
to 'arouse' him into satisfactory intercourse. Neuropathy (e.g. diabetes) or other nerve
damage (e.g. radical prostatectomy) is less likely to respond to PDE5 depending upon the extent of
nerve damage.
|
|
Figure 1. Physiology of
erection
The first PDE5 inhibitor sildenafil (Viagra) became available in 1998. Goldstein et.
al. (8) first demonstrated its efficacy and safety. Four years of clinical experience as first line therapy has confirmed
that sildenafil is successful in treating overall 70% of patients with


|