|
Intracavernosal injections containing phentolamine and papaverine with or without alprostadil
are also available. Patients should be warned about priapism and advised on initial management
with moderate exercise and decongestant tablets and to seek medical advice if priapism persists
after 4-6 hours.
Transurethral alprostadil therapy is rarely used in Australia. Clinically it was only approximately
30% effective and not uncommonly caused urethral burning and penile and testicular
pain.(9)
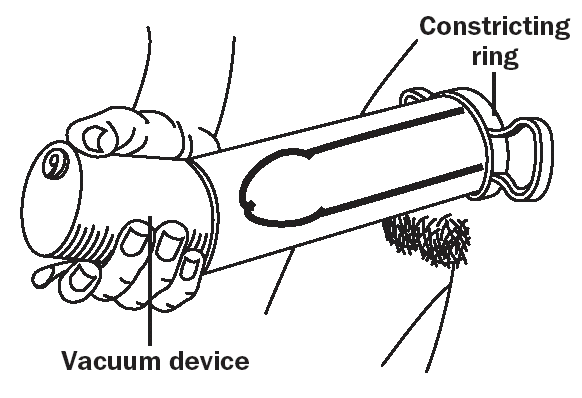
Vacuum erection devices
Vacuum devices can be useful for patients with chronic or occasional organic or psychogenic ED or
where other treatments have failed, and may be used together with other ED therapies. Figure 3
demonstrates the use of a vacuum device. The erect
penis is bluish in colour and cool to touch. Side effects include pain, numbness, bruising and a sense
of altered ejaculation. Cooperation by the partner is required and drop out rates tend to be high.
Figure 3. The vacuum device is placed over the penis,
subsequent vacuum draws blood into the penis: the constructor ring is rolled onto the base of the penis
and the device is removed from the engorged penis.
|
|
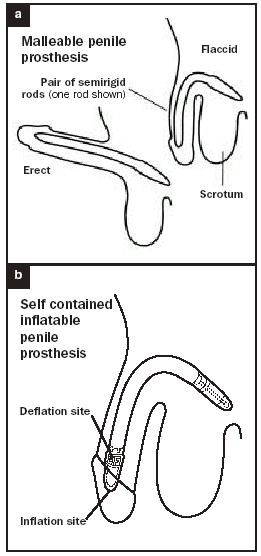
Surgical implants
Men with severe ED not responding to other treatments may opt for surgical implants. Different types
of prostheses are available, ranging from malleable rods (Figure 4a, b) to inflatable tubes that mimic the
function of the corpora cavernosa (Figure 5) and semi-rigid devices. Surgery is quite expensive and
complications such as mechanical failures and infection can occur even years later. Urologists with a
particular interest in this area and in other forms of penile surgery for ED (severe Peyronies, re-establishment
of penile vascular supply following pelvic trauma) should be consulted.
Figure 4a, b. Penile prosthetic implants
a. Malleable rod b. Inflatable implant


|