 Feedback Question 3
Feedback Question 3
Feedback Question 3
Selection 1
Haemoglobin and film, looking for a picture of anaemia with iron deficiency
-
Correct. If symptoms of anaemia are present a diagnosis should be confirmed,
including the type, the cause and the severity. A history of prolonged blood
loss without symptoms of anaemia should also have a Hb and a film ordered.
Selection 2
A Pap smear to rule out cervical intraepithelial neoplasia (CIN) as a cause of
menorhaggia -
Correct. A Pap smear should always be carried out on any woman who is due for
one, when they are having a vaginal examination, or on any woman who has
abnormal bleeding. However, when the problem is menorrhagia it is most unlikely
that a Pap smear would confirm a diagnosis or influence treatment.
Selection 3
D & C and hysteroscopy
Correct. This is the traditional 'gold standard' for diagnosing menorrhagia. A
hysteroscopy enables visualisation of the uterine cavity. A curettage can then
be carried out to obtain a histological sample to send to pathology. A D & C
alone is no longer adequate. A curettage can be compared to walking into a dark
room and feeling the walls whereas a hysteroscopy is like standing at the door,
turning on the light and entering the room.
Click here to view a video of hysteroscopy
Selection 4
Outpatient hysteroscopy with endometrial sampling -
Incorrect. Outpatient hysteroscopy and endometrial sampling could be used. This
is probably a better method for assessing women with inter-menstrual bleeding
rather than menorrhagia. When menorrhagia is present thorough endometrial
histology needs to be performed to diagnose any hy[erplasia and/or atypia. This
is better done by formal curettage than by endometrial sampling.
Selection 5
Pelvic ultrasound -
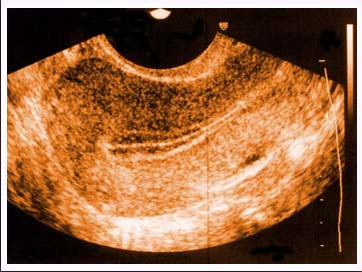
Incorrect. Pelvic ultrasound may be of some help, measuring the size of the
uterus and detecting fibroids but it is a relatively expensive test and not as
good as vaginal examination. It does have the advantage of visualising the
ovaries quite well.