|
Suicide pattern in Kermanshah
Province, West of Iran:
March 2012- March 2013
Mehran Rostami
(1)
Abdollah Jalilian (2)
Ramin Rezaei-Zangeneh (3)
Teimour Jamshidi (4)
Mohsen Rezaeian (5,6)
(1) Mehran Rostami (MSc); Deputy for Treatment,
Kermanshah University of Medical Sciences, Kermanshah,
Iran
(2) Abdollah Jalilian (PhD); Department of Statistics,
Razi University, Kermanshah, Iran
(3) Ramin Rezaei-Zangeneh (MD); Deputy for Treatment,
Kermanshah University of Medical Sciences, Kermanshah,
Iran
(4) Teimour Jamshidi (BSc); Head of Research
and Training in Forensic Medicine Organization
of Kermanshah province, Kermanshah, Iran
(5) Epidemiology and Biostatistics Department,
Rafsanjan Medical School, Rafsanjan University
of Medical Sciences, Rafsanjan, Iran.
(6) Occupational Environmental Research Center,
Rafsanjan University of Medical Sciences, Rafsanjan,
Iran
Corresponding author:
Professor
Mohsen Rezaeian (PhD)
Epidemiology and Biostatistics Department, Occupational
Environmental Research Center
Rafsanjan Medical School, Rafsanjan University
of Medical Sciences, Rafsanjan-Iran
Tel: +983434331315
Fax: +983434331315
Email: moeygmr2@yahoo.co.uk
|
Abstract
Background:
Kermanshah
province (the most populated province
in the west of Iran) has one of the highest
suicide rates among Iran's provinces.
This study aims to update the existing
knowledge of suicide situations in the
province in order to take the first step
towards designing preventive interventions.
Methods:
Data were extracted from the electronic
files of the Forensic Medicine Organization
(FMO) of Kermanshah province during the
course of one-year. The chi-squared test
and Cramer's V statistic were used to
assess the associations between the demographic
variables.
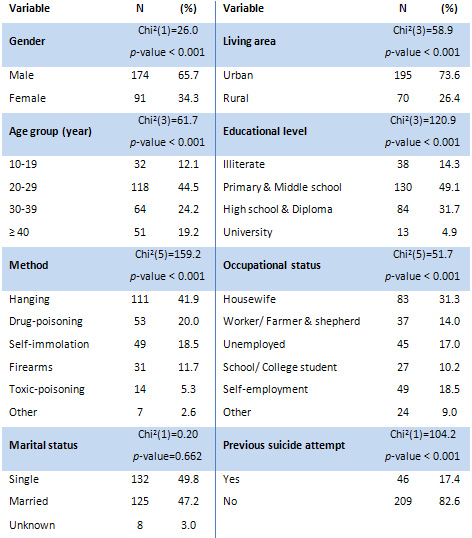
Results: 265
confirmed cases (65.7% males and 34.3%
females) of suicide were registered during
the study period. The overall annual rate
of suicide in Kermanshah province was
13.6 persons per 100,000 residents. Approximately,
45% of the cases were between 20 and 29
years old. Hanging in males (50%) and
self-immolation in females (43%) were
the dominant suicide methods.
Conclusion: Compared
to the average suicide rate in Iran, Kermanshah
province has a noticeably higher rate.
Focusing on social determinants of health
in the population should be seriously
considered by the health system's policy-makers
regarding practical approaches to be used
for the purposes of reducing suicide.
Key words:
Measure of association, Social determinants
of health, Suicide, Iran
|
Suicide is one of the most complex aspects
of human behavior where a person ends his/her
life with a deliberate and conscious effort
(1, 2). According to suicide statistics reported
to World Health Organization (WHO), suicide
rates vary greatly among countries (3). There
are several problems and difficulties in accurately
defining, measuring, recording, reporting and
scientific studying of suicide (4). Most of
the problems are related to social stigma associated
with this phenomenon which is prevalent, more
or less, in every community (2). Also, the official
suicide registration system in different communities
varies (3, 5), including in Iran (6, 7). Furthermore,
in some communities, more than one organization
is active in identification and registration
of suicide data and this issue can cause obvious
differences between statistics submitted on
suicide cases (2, 7).
In Iran, suicide has shown an increasing trend
from 1990 to 2010 (8, 9) and distribution of
suicide mortality across the country is more
prevalent among the western provinces (10).
Based on the information obtained from the death
registration system of the Ministry of Health
and Medical Education, the statistics related
to completed suicide in the first nationwide
study of mortality profile in 29 provinces of
the country in 2004 showed that Kermanshah province
accounted for 14.0 per 100,000 and stood at
the 3rd place in the country in terms of high
rates of mortality caused by suicide. It should
be mentioned that the said national average
has been estimated as much as 5.2 per 100,000
in the same year (11). Moreover, Kermanshah
province was second highest in terms of suicide
mortality rate in the country during 2006-2010
(10). Another nationwide study of mortality
profile in 29 provinces of the country in 2010
showed that hanging and self-immolation stood
at 5th place among the leading causes of death
among males and females aged from 15 to 49 years,
respectively (12).
With due observance to the above-mentioned subjects,
analyzing the current situation of suicide among
various age and gender groups of people in Kermanshah
province and evaluating the suicide rates in
these groups are the main objectives of this
study. Based on this issue, not only can the
vulnerable groups be identified, but also a
giant stride can be taken in this province in
order to reduce rates of suicide through updating
knowledge and information required for healthcare
and medical treatment planning and to use the
results to take the first step towards designing
preventive interventions and mental health promotion.
Ethics Statement
Before reviewing data, burial permit number,
name and surname of the deceased were omitted
due to respect to the principle of medical secrecy.
No private information of the deceased who committed
suicide was used in conducted analysis and obtained
results and hence no informed consent was required
for this study. The study protocol was approved
by the research committee of Kermanshah University
of Medical Sciences (No. 93213).
Socio-demographic Characteristics
Kermanshah province is the most populated province
in the west of Iran with 14 counties, 31 cities
and towns and 86 rural districts. Based on the
2011 Census of Population and Housing, Kermanshah
province has 1,945,227 people and accounts for
2.7% share of total population of the country
with approximately 70% of urbanization rate
and nearly 16% of unemployment rate (13).
Data source
In this cross-sectional study; electronic files
of confirmed committed suicide data of the Forensic
Medicine Organization (FMO) of Kermanshah province
collected from March 21, 2012 to March 20, 2013
were used. This electronic file contains the
following variables: death time, permanent residence
of the deceased including urban or rural regions.
Suicide methods included hanging, self-immolation,
firearms, intentional drug-poisoning, self-poisoning
from toxic substances (toxic-poisoning), and
others. The other methods category included
cutting, drowning, jumping from a high place,
and other unspecified means. The age of the
deceased has been calculated according to birth
year. It is worth mentioning that all identified
cases were older than 10 years of age at the
time of the committed suicide; hence, the age
variable was grouped in four categories including
10-19 years, 20-29 years, 30-39 years, and 40
years and above. Marital status consisted of
single, married and unknown. Educational status
was classified into four groups: illiterate,
primary and middle schools, high school and
diploma, and university degrees. Previous history
of attempting suicide includes yes, and no options.
Consistent with previous researchers, occupational
status variable was grouped in six categories
including: housewife, worker and farmer, unemployed
people, school/college student, self-employment
and others (military man, soldier, driver, retired,
other businesses and so on).
To accurately evaluate the incidence rate of
suicide in Kermanshah, the first important step
was to determine some criteria for inclusion
in the study. For example, an autopsy performed
in one of the forensic medical centers in the
province by a forensic pathologist to determine
the cause of death was not a sufficient inclusion
criterion for participating in the study. Therefore,
the cases indicating permanent postal address
of the deceased person living in one of the
cities or villages at the jurisdiction of Kermanshah
province were analyzed in this study. Also,
to quantify the data, the common procedure for
recording the suicide cases was modified in
this study to the effect that when the subjects
of the study were diagnosed with the death caused
by suicide using medical examination and pathological
tests, the number of subjects of the study was
registered in statistical forms of the suicide
data of the same month; i.e., if the result
of pathological tests of a person verifies that
he/she has died due to suicide several months
after the real time of death, the relevant information
is recorded in the statistics related to the
month when the result is specified and not in
the statistics of the real time of death. Thus,
to correct this procedure and prevent misclassification
bias in data analysis, the researcher had to
reset the statistics of suicide cases based
on the real time of death. The above-mentioned
modifications resulted in the improvement of
the quality of the numerator of annual suicide
rates.
Incidence rates were calculated as the number
of suicide cases divided by the corresponding
estimated population, multiplied by 100,000.
The population of Kermanshah province estimation
extracted from provincial statistical yearbook
for 2013 was used as denominators.
Data analysis
We first examined the distribution of completed
suicide within each of the independent variable
categories. The Pearson's chi-square test of
independence at the 0.05 significance level
and the Cramer's V measure of association were
used to assess the associations between each
pair of the demographic variables. The Cramer's
V statistic varies from 0 (no association) to
1 (complete association) and measures the strength
of relationship between nominal variables. According
to this method, qualitative descriptions are
associated with the following intervals: less
than or equal to 0.40, poor agreement; 0.41-0.60,
moderate agreement; 0.61-0.80, good agreement;
0.81-1.00, excellent agreement (14). All statistical
analyses were conducted using Stata software
version 12 (StataCorp LP, College Station, TX,
USA).
Table
1:
Demographic
characteristics
of
completed
suicide
cases
in
Kermanshah
province,
Iran
(March
2012
to
March
2013)
Table
2:
Suicide
methods
among
completed
suicide
cases
by
gender
and
living
area,
Kermanshah
province,
Iran
(March
2012
to
March
2013)
Click
here
for
Table
3:
Chi-squared
statistic
and
p-value
for
the
test
of
independence
between
the
variables
with
their
corresponding
Cramer's
V
measure
of
association
Click
here
for
Table
4:
Absolute
frequency
and
percentage
of
completed
suicide
according
to
days
of
week,
Kermanshah
province,
Iran
(March
2012
to
March
2013)
Click
here
for
Figure
1:
Age-distribution
of
completed
suicide
cases
by
suicide
methods,
Kermanshah
province,
Iran
(March
2012
to
March
2013)
Click
here
for
Figure
2:
Annual
rates
of
completed
suicides
according
to
the
counties,
Kermanshah
province,
Iran,
March
2012
to
March
2013
(ranked
by
suicide
mortality
rate).
A
total
of
265
confirmed
cases
of
death
by
suicide
have
been
registered
from
March
2012
to
March
2013
in
the
population
residing
in
Kermanshah
province,
including
174
men
(65.7%)
and
91
women
(34.3%)
with
a
mean
age
of
31.3±14
years
(Mean±SD).
The
sex
ratio
(male-to-female)
of
the
deceased
stands
at
1.9:1
and
more
than
91%
of
women
were
housewives.
In
addition,
195
persons
(73.6%)
and
70
persons
(26.4%)
of
the
deceased
resided
in
urban
and
rural
regions,
respectively.
There
is
no
significant
difference
(Chi2(1)=0.2,
p-value=0.662)
between
married
and
single
deceased
(excluding
8
cases
with
unknown
marital
status).
More
detailed
information
about
variables
related
to
the
completed
suicide
cases
are
presented
in
Table
1.
For
example,
it
can
be
observed
that
approximately
45%
of
the
deceased
who
committed
suicide
were
in
the
20-29
year
age
group.
Since
the
provincial
statistical
yearbook
had
no
estimates
for
the
population
of
the
province
in
each
age
group
during
the
study
period,
calculation
of
suicide
rate
in
each
age
group
was
impossible.
Nevertheless,
Figure
1
shows
the
absolute
frequency
of
suicide
methods
by
age
groups.
It
can
be
seen
that
intentional
drug-poisoning
is
notably
higher
in
the
20-29
age
group.
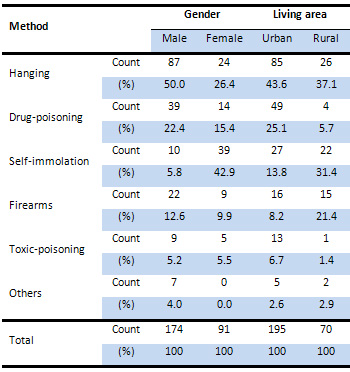
The
absolute
frequency
and
percentage
of
suicide
methods
by
gender
and
living
area
are
presented
in
Table
2.
Overall,
the
most
common
suicide
methods
in
Kermanshah
province
were
hanging
(42%)
followed
by
intentional
drug-poisoning
(20%),
and
self-immolation
(18.5%).
The
most
common
suicide
method
was
hanging
(50%)
for
men
and
self-immolation
(43%)
for
women.
Based
on
contents
of
this
table,
68.4%
of
males
have
committed
suicide
using
violent
methods
(hanging,
self-immolation,
firearms)
and
79.1%
of
females
have
committed
suicide
using
the
same
three
violent
methods.
The
overall
annual
suicide
rate
in
Kermanshah
province
is
estimated
at
13.6
per
100,000
residents
during
the
study
period.
Figure
2
shows
the
annual
suicide
rate
of
each
county
of
the
province.
This
figure
shows
that
Qasr-e
Shirin
county
with
27.2
and
Harsin
county
with
7.0
per
100,000
residents
respectively
have
the
highest
and
lowest
annual
suicide
rate
in
the
province.
Thus,
there
is
an
almost
four
times
difference
between
incidences
of
suicide
in
these
counties.
Results
of
Pearson's
chi-square
tests
and
Cramer's
V
values
are
reported
in
Table
3.
According
to
the
results,
suicide
method
is
significantly
associated
with
gender,
living
area,
occupation,
age
group,
education
and
marital
status.
The
corresponding
Cramer's
V
values
indicate
that
the
association
between
suicide
method
and
gender
is
stronger
than
the
association
between
suicide
method
and
any
other
factor.
Similarly,
we
can
see
that
gender
is
significantly
associated
with
occupation,
education,
marital
status
and
living
area.
More
than
17%
of
the
deceased
had
a
history
of
previous
suicide
attempts
but
there
was
no
statistically
significant
association
between
history
of
previous
suicide
attempts
and
other
variables
of
the
study.
Table
4
shows
the
frequency
and
percentage
of
committed
suicide
in
weekdays.
According
to
this
table,
although
Monday
has
a
slightly
higher
frequency
based
on
the
chi-square
test
for
homogeneity,
there
is
no
statistically
significant
difference
(Chi2(6)=12.44,
p-value=0.053)
between
the
frequencies
of
suicide
in
different
weekdays.
As
it
is
observed
from
results
of
this
study,
completed
suicide
has
been
focused
on
in
the
present
study.
The
completed
suicide
statistics
had
appropriate
reliability,
because
the
records
and
reports
of
the
death
due
to
completed
suicide
had
higher
accuracy
in
comparison
to
attempted
suicide
statistics
(15,
16).
Based
on
the
obtained
results,
the
overall
annual
rate
of
completed
suicide
in
this
province
stood
at
13.6
persons
per
100,000
people,
and
suicide
rate
was
observed
more
in
urban
regions
than
rural
regions.
One
of
the
most
important
causes
for
this
event
could
be
increased
level
and
rate
of
urbanization
in
the
province
as
a
result
of
rapid
migration
of
rural
inhabitants
to
urban
areas.
Such
change
in
the
living
environment
has
not
been
adequately
coupled
with
concomitant
cultural
adaptation.
In
this
regard,
the
completed
suicide
rate
in
this
province
is
much
higher
than
that
of
the
national
suicide
rate
(10,
17,
18).
Some
of
the
main
reasons
for
the
high
rate
of
committing
suicide
in
western
provinces
of
Iran
have
been
mentioned
in
previous
research
(2,
7,
10,
17).
The
ratio
of
males
who
died
by
suicide
was
higher
than
that
of
females,
so
this
finding
is
consistent
with
the
results
of
previous
studies
(16).
The
present
study
showed
that
the
majority
of
the
females
who
committed
suicide
were
housewives.
The
reason
for
that
is
most
middle-
and
old-aged
females
in
Iran
are
housewives
without
income.
Therefore,
it
seems
rational
that
the
majority
of
the
females
who
committed
suicide
are
housewives
(16).
The
noticeable
point
is
that
Kermanshah
province
stood
at
the
3rd
place
in
the
country
in
2004
in
terms
of
death
rate
due
to
suicide,
while
four
counties
of
Sarpol-e
Zahab,
Sahneh,
Harsin
and
Qasr-e
Shirin
(all
located
in
Kermanshah
province)
were
among
the
highest
death
rate
caused
by
suicide
across
the
country
(11).
In
the
present
study,
three
counties
of
Qasr-e
Shirin,
Sarpol-e
Zahab
and
Sahneh
are
among
the
highest
suicide
rate
yet
(approximately
20
persons
per
100,000
residents
and
higher).
High
unemployment
rate
in
this
province,
compared
to
the
other
provinces,
has
been
cited
as
one
of
the
main
probable
reasons
for
the
high
rate
of
suicide
in
Kermanshah
province.
Of
course,
relationship
between
economic
problems
and
unemployment
with
suicide
in
Kurdish
ethnicity
has
previously
been
mentioned
(16,
17,
19,
20).
As
mentioned,
hanging
and
self-immolation
are
the
main
methods
of
committing
suicide
among
males
and
females
respectively;
this
finding
is
consistent
with
the
pattern
of
suicide
methods
observed
in
previous
years
in
this
province
(16)
and
also
with
the
governing
pattern
on
the
whole
country
(21,
22)
and
in
Middle
Eastern
countries
(23).
Based
on
this
study,
intentional
drug-poisoning
is
the
2nd
most
common
method
that
leads
to
deaths
due
to
suicide.
This
method
is
frequently
used
in
young
female
attempters
and
also
is
one
of
the
main
methods
of
suicide
in
males
(24).
Frequently
use
of
violent
methods
in
western
provinces
of
the
country
such
as
Kermanshah
province
may
be
due
to
post-war
problems
between
the
Iran
and
Iraq.
This
is
an
important
issue
since,
the
outbreak
of
the
Iran-Iraq
war
in
most
parts
of
western
provinces
of
the
country
including
Kermanshah
province
has
been
cited
as
the
one
of
the
main
reasons
for
occurrence
of
violent
behaviors
including
suicide
(19,
25).
The
reasons
for
the
high
incidence
of
suicide
by
hanging
have
been
studied,
the
results
of
which
indicate
that
hanging
is
a
more
acceptable
method,
and
death
caused
by
hanging
is
less
likely
to
be
misclassified
in
the
death
group
with
ambiguous
reasons
or
accidental
death
due
to
the
transparency
of
death
method
(24,
26).
If
we
study
self-immolation
as
the
main
cause
of
death,
it
can
be
mentioned
that
this
aggressive
and
violent
suicide
method
is
mostly
common
in
developing
countries
such
as
Iran
and
other
Middle
Eastern
countries
(2,
24,
27).
Among
the
main
factors
that
influence
the
acceptability
of
suicide
by
self-immolation,
we
can
refer
to
Kurdish
ethnicity,
female
gender,
young
adult
age
(19),
adjustment
disorder
(19,
28,
29),
cultural
differences
in
attitude
towards
self-immolation,
storage
and
accessibility
of
inflammable
liquids
at
home
and
also
storage
of
kerosene
at
home
for
cooking
usage
(18).
All
of
these
factors
play
an
important
role
in
highlighting
this
violent
suicide
method
in
Kermanshah
province
and
even
"copycat"
phenomenon
can
be
influential
with
regard
to
the
acceptability
of
this
violent
suicide
method
(17).
It
should
be
kept
in
mind
that
like
other
societies
suicide
is
a
phenomenon
that
conflicts
with
religious
and
socio-cultural
values
in
Iran
(2,
15,
20);
so
the
true
suicide
incidence
rate
might
have
been
underestimated
(16).
Undoubtedly,
increasing
mutual
cooperation
and
collaboration
among
official
organizations
involved
in
registration
of
suicide
statistics
is
one
of
the
most
effective
measures
to
promote
quality
of
death
registration
system's
data
in
Iran
(6).
Our
results
furthermore
highlighted
that
most
cases
of
suicide
in
this
province
occur
in
age
group
of
20-29
years.
Also
this
finding
is
consistent
with
the
results
of
previous
studies
(9,
16,
17,
25,
27,
30),
and
the
average
age
of
the
study
subjects
at
the
time
of
death
is
similar
to
the
age
of
the
deceased
from
completed
suicide
in
this
province
(11).
It
should
be
noted
that
the
previous
history
of
attempting
suicide
is
one
of
the
recognized
risk
factors
of
subsequent
suicide
(18,
31).
In
this
study,
more
than
17%
of
the
deceased
caused
by
suicide
had
a
previous
history
of
attempting
suicide,
so
that
activation
of
mental
health
services
after
attempting
suicide
for
the
doer
and
his/her
family
(15,
31)
is
similar
to
launching
an
online
telephone
line
by
psychiatrist
or
hospital
admissions
for
high
risk
cases
(31)
which
can
play
an
important
role
in
prevention
of
re-attempting
suicide
coupled
with
reduced
rate
of
suicide
as
well.
In
western
countries,
most
suicide
cases
occur
on
Mondays
and
Tuesdays
(32,
33).
In
our
study,
there
is
no
significant
difference
among
the
frequencies
of
suicide
in
weekdays.
It
should
be
noticed
that
the
pattern
observed
in
western
countries
may
be
related
to
the
early
days
of
the
business
weeks
but
Monday
in
Iran
is
the
middle
of
the
weekdays.
The
pattern
should
be
taken
into
reconsideration
within
the
longer
time
frame
using
suicide
data
of
other
regions
of
the
country.
Considering
the
above-mentioned
issues,
substantial
efforts
for
preventing
suicides
are
needed
in
western
provinces
of
the
country
(10,
18).
The
policymakers
of
the
health
system
of
the
country
must
seriously
take
into
consideration
the
revision
of
suicide
prevention
programs
and
treatment
of
mental
and
reactive
disorders,
especially
major
depression,
substance
use
disorders,
bipolar
disorders,
mood
and
anxiety
disorders
(9).
We
further
suggest
that
more
information
needs
to
be
gathered
specially
within
suicide
prevention
programs.
These
might
at
the
very
least
include:
"the
causes
for
suicide",
"any
preceding
psychological
disorders
among
suicidal
cases"
and
"the
types
of
any
medical
treatment
they
received".
The
following
are
considered
as
the
main
reasons
influence
on
the
increase
in
suicide
cases
in
the
Middle
Eastern
countries:
Lack
of
success
of
regional
countries
in
accurate
and
suitable
transfer
of
Islamic
values
and
principles
to
the
young
generation;
superficial
attention
to
the
Islamic
rules
and
not
paying
due
attention
to
the
depth
of
these
rules
(such
as
inattention
to
the
fair
distribution
of
wealth
in
society
and
its
role
in
prevention
of
suicide);
inferior
position
of
women
in
some
Middle
Eastern
countries
dating
back
to
the
old
culture
and
tradition
of
the
countries,
such
as
forced
marriage
(23).
It
can
be
understood
easily
that
suicide
is
a
very
complex
and
multidimensional
problem
and
tackling
this
problem
requires
joint
efforts
of
all
people,
society
and
governments.
There
are
several
practical
strategies
to
reduce
the
completed
suicide
rate
and
to
promote
the
mental
health
of
society
across
the
province.
All
of
these
effective
strategies
and
community-based
interventions
should
be
taken
into
consideration
by
policy-makers
of
the
health
system
to
reduce
the
incidence
of
suicide
in
the
west
of
Iran:
-
Paying
enough
attention
to
enhancing
social
equity
and
alleviation
of
economic
problems
and
unemployment
rate;
-
Dissemination
of
culture
of
simple
living
in
society,
especially
among
young
couples;
-
Increasing
the
number
of
family
counseling
centers
and
training
at-risk
individuals
about
coping
skills;
-
Making
effort
in
line
with
promoting
position
of
females
in
society
with
emphasis
on
increasing
participation
of
women
in
the
workforce;
-
Making
effort
in
line
with
adjusting
conflicts
as
a
result
of
incongruousness
and
clash
of
modern
and
traditional
values.
The
authors
would
like
to
thank
Mr.
Shahab
Rezaeian
(PhD
student
of
Epidemiology,
Shiraz
University
of
Medical
Sciences,
Iran)
and
Mrs.
Hadis
Asadi
(MSc
of
Nursing);
as
well
as
the
chairman
and
personnel
of
Imam
Khomeini
hospital
(Eslamabad-e
Gharb,
Kermanshah,
Iran)
for
their
collaboration
throughout
this
work.
1.
Bertolote
JM,
Wasserman
D.
Development
of
definitions
of
suicidal
behaviours.
In:
Wasserman
D,
Wasserman
C,
editors.
Oxford
Textbook
of
Suicidology
and
Suicide
Prevention.
1
ed.
New
York:
Oxford
University
Press;
2009.
p.
87-90.
2.
Rezaeian
M.
Epidemiology
of
Suicide.
In:
Hatami
H,
Razavi
SM,
Eftekhar
AH,
Majlesi
F,
Sayed
Nozadi
M,
Parizadeh
SM,
editors.
Textbook
of
Public
Health.
3rd
ed.
Tehran:
Arjmand
publications;
2013.
p.
1968-93.
3.
Liu
KY.
Suicide
Rates
in
the
World:
1950-2004.
Suicide
Life
Threat
Behav.
2009;39(2):204-13.
4.
Rezaeian
M.
Methodological
issues
and
their
impacts
on
suicide
studies.
Middle
East
J
Business.
2012;7(2):17-9.
5.
Hawton
K,
van
Heeringen
K.
Suicide.
Lancet.
2009;373(9672):1372-81.
6.
Jafari
N,
Kabir
MJ,
Motlagh
ME.
Death
Registration
System
in
I.R.Iran.
Iranian
J
Publ
Health.
2009;38(1):127-9.
7.
Rezaeian
M.
Comparing
the
Statistics
of
Iranian
Ministry
of
Health
with
Data
of
Iranian
Statistical
Center
Regarding
Recorded
Suicidal
Cases
in
Iran.
J
Health
Syst
Res.
2013;8(7):1190-6.
8.
Forouzanfar
MH,
Sepanlou
SG,
Shahraz
S,
Dicker
D,
Naghavi
P,
Pourmalek
F,
et
al.
Evaluating
causes
of
death
and
morbidity
in
Iran,
global
burden
of
diseases,
injuries,
and
risk
factors
study
2010.
Arch
Iran
Med.
2014;17(5):304-20.
9.
Naghavi
M,
Shahraz
S,
Sepanlou
SG,
Dicker
D,
Naghavi
P,
Pourmalek
F,
et
al.
Health
transition
in
Iran
toward
chronic
diseases
based
on
results
of
Global
Burden
of
Disease
2010.
Arch
Iran
Med.
2014;17(5):321-35.
10.
Kiadaliri
AA,
Saadat
S,
Shahnavazi
H,
Haghparast-Bidgoli
H.
Overall,
gender
and
social
inequalities
in
suicide
mortality
in
Iran,
2006-2010:
a
time
trend
province-level
study.
BMJ
Open.
2014;4(8):e005227.
11.
Naghavi
M,
Jafari
N.
Mortality
profile
for
29
provinces
of
Iran
(2004).
Tehran:
Iranian
Ministry
of
Health
and
Medical
Education-Deputy
of
Health;
2007.
12.
Khosravi
A,
Aghamohamadi
S,
Kazemi
E,
Pourmalek
F,
Shariati
M.
Mortality
Profile
in
Iran
(29
Provinces)
over
the
Years
2006
to
2010.
Tehran:
Ministry
of
Health
and
Medical
Education;
2013.
p.
413-4.
13.
Statistical
Center
of
Iran.
Population
and
housing
census
2011
Tehran2011
[2015
Mar
10].
Available
from:
http://www.amar.org.ir/Default.aspx?tabid=1208].
14.
Liebetrau
AM.
Measures
of
association.
Beverly
Hills,
CA:
Sage
Publications
Inc,;
1983.
15.
Najafi
F,
Hasanzadeh
J,
Moradinazar
M,
Faramarzi
H,
Nematollahi
A.
An
epidemiological
survey
on
the
trends
of
the
suicide
incidence
in
the
southwest
Iran,
2004-2009.
Int
J
Health
Policy
Manag.
2013;1(3):219-22.
16.
Poorolajal
J,
Rostami
M,
Mahjub
H,
Esmailnasab
N.
Completed
suicide
and
associated
risk
factors:
a
six-year
population
based
survey.
Arch
Iran
Med.
2015;18(1):39-43.
17.
Ahmadi
AR.
Suicide
by
self-immolation:
comprehensive
overview,
experiences
and
suggestions.
J
Burn
Care
Res.
2007;28(1):30-41.
18.
Ghafarian-Shirazi
HR,
Hosseini
M,
Zoladl
M,
Malekzadeh
M,
Momeninejad
M,
Noorian
K,
et
al.
Suicide
in
the
Islamic
Republic
of
Iran:
an
integrated
analysis
from
1981
to
2007.
East
Mediterr
Health
J.
2012;18(6):607-13.
19.
Ahmadi
A,
Mohammadi
R,
Stavrinos
D,
Almasi
A,
Schwebel
DC.
Self-Immolation
in
Iran.
J
Burn
Care
Res.
2008;29(3):451-60.
20.
Groohi
B,
Rossignol
AM,
Barrero
SP,
Alaghehbandan
R.
Suicidal
behavior
by
burns
among
adolescents
in
Kurdistan,
Iran.
Crisis.
2006;27(1):16-21.
21.
Saberi-Zafarghandi
MB,
Hajebi
A,
Eskandarieh
S,
Ahmadzad-Asl
M.
Epidemiology
of
suicide
and
attempted
suicide
derived
from
the
health
system
database
in
the
Islamic
Republic
of
Iran:
2001-2007.
East
Mediterr
Health
J.
2012;18(8):836-41.
22.
Shojaei
A,
Moradi
S,
Alaeddini
F,
Khodadoost
M,
Barzegar
A,
Khademi
A.
Association
between
suicide
method,
and
gender,
age,
and
education
level
in
Iran
over
2006-2010.
Asia
Pac
Psychiatry.
2014;6(1):18-22.
23.
Rezaeian
M.
Suicide
in
the
middle-eastern
countries:
Introducing
the
new
emerging
pattern
and
a
framework
for
prevention.
Middle
East
J
Business.
2014;9(3):45-6.
24.
Leenaars
AA,
Lester
D.
Domestic
integration
and
suicide
in
the
provinces
of
Canada.
Crisis:
The
Journal
of
Crisis
Intervention
and
Suicide
Prevention.
1999;20(2):59.
25.
Alaghehbandan
R,
Lari
AR,
Joghataei
M-T,
Islami
A,
Motavalian
A.
A
prospective
population-based
study
of
suicidal
behavior
by
burns
in
the
province
of
Ilam,
Iran.
Burns.
2011;37(1):164-9.
26.
Razaeian
M,
Mohammadi
M,
Akbari
M,
Maleki
M.
The
most
common
method
of
suicide
in
Tehran
2000-2004:
implications
for
prevention.
Crisis.
2008;29(3):164-6.
27.
Rezaeian
M.
Suicide
among
young
middle
eastern
muslim
females.
Crisis.
2010;31(1):36-42.
28.
Ahmadi
A,
Mohammadi
R,
Schwebel
DC,
Yeganeh
N,
Hassanzadeh
M,
Bazargan-Hejazi
S.
Psychiatric
disorders
(Axis
I
and
Axis
II)
and
self-immolation:
a
case-control
study
from
Iran.
J
Forensic
Sci.
2010;55(2):447-50.
29.
Ahmadi
A,
Mohammadi
R,
Schwebel
DC,
Yeganeh
N,
Soroush
A,
Bazargan-Hejazi
S.
Familial
risk
factors
for
self-immolation:
a
case-control
study.
J
Womens
Health
(Larchmt).
2009;18(7):1025-31.
30.
Amiri
B,
Pourreza
A,
Rahimi-Foroushani
A,
Hosseini
SM,
Poorolajal
J.
Suicide
and
associated
risk
factors
in
Hamadan
province,
west
of
Iran,
in
2008
and
2009.
J
Res
Health
Sci.
2012;12(2):88-92.
31.
Schwartz-Lifshitz
M,
Zalsman
G,
Giner
L,
Oquendo
MA.
Can
we
really
prevent
suicide?
Curr
Psychiatry
Rep.
2012;14(6):624-33.
32.
Ajdacic-Gross
V,
Tran
US,
Bopp
M,
Sonneck
G,
Niederkrotenthaler
T,
Kapusta
ND,
et
al.
Understanding
weekly
cycles
in
suicide:
an
analysis
of
Austrian
and
Swiss
data
over
40
years.
Epidemiol
Psychiatr
Sci.
2014;23:1-7.
[Epub
ahead
of
print].
33.
Miller
TR,
Furr-Holden
CD,
Lawrence
BA,
Weiss
HB.
Suicide
deaths
and
non-fatal
hospital
admissions
for
deliberate
self-harm:
temporality
by
day
of
week
and
month
of
year,
United
States.
Crisis.
2012;33(3):169-77.
|

