|
|
 |
Medicine and Society
........................................................
Clinical Research and
Methods
.......................................................
Education
and Training
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| October 2014 -
Volume 12 Issue 8 |
|
Successful
use of 0.2% Glyceryl Trinitrate ointment for anal
fissures in Erbil city, Iraq
Abdulqadir
M. Zangana (1)
Kawa F. Dizaye (2)
(1) Professor of Surgery, CABS-FICS-MD,
Head of Department of surgery, Consultant Surgeon,
College of Medicine, Hawler Medical University,
Iraq.
(2) Professor of Pharmacology, HD, MSc, PhD,
Head of department of Pharmacology College of
Medicine, Hawler Medical University, Iraq.
Correspondence:
Dr. Kawa Dizaye, Professor of Pharmacology,
Hawler Medical University, Erbil, Iraq
Tel: 009647504452392.
Email: doctorkawa@gmail.com
|
Abstract
Aim
of the study:
To assess the clinical efficacy of 0.2%
glyceryl trinitrate ointment in the management
of acute and chronic anal fissures.
Patients and Methods: A prospective
clinical study conducted on consecutive
patients presented to the surgical clinic
of Erbil teaching Hospital, Erbil city
with acute and chronic anal fissures,
from June 2009 till August 2012.
These patients were treated with topical
0.2% glyceryl trinitrate (GTN) paste in
soft white paraffin three times a day.
Patients were examined at regular intervals
to evaluate the fissure status, adverse
reactions, symptomatic control and recurrence.
One hundred and fifty nine patients with
acute and chronic anal fissures were evaluated
in the study. Fifty one of them were lost
to follow-up and 108 were remaining (94.7%)
Results: At
the end of complete course (6-8 weeks),
pain was completely relieved in 80.9 %
and partially better in 7.4%, bleeding
was absent in 83.7%, anal tone became
normal in 80%, and in 80.3 % had healing.
The course was completed or taken for
longer duration in patients 62.9%. GTN
was stopped before end of the course in
40 patients (37%) due to different causes,
side effects mainly headache 60 %, non
compliance 95%, or no response at all
50%. Recurrence of symptoms in the first
six months was seen in 26 patients. It
was seen that in two-thirds of the cases,
the duration of treatment was less than
6-8 weeks. There was a highly significant
positive relationship between duration
of treatment and recurrence of symptoms.
The recurrence was treated surgically
in 53% patients, traditional ointments
in 30.8% patients, and repeated GTN course
in 15.4% patients.
Conclusion: The use of 0.2% GTN
ointment induces rapid healing of anal
fissures with an 80.3% healing rate in
this study. Successful treatment may come
at the expense of high incidence of headache
although it is lower in our study due
to lower GTN concentration.
Key words: Glyceryl
trinirate 0.2% ointment, acute and chronic
anal fissures
|
Anal fissure is a benign painful condition of
the anoderm. Raised resting internal anal sphincter
pressure is important in the pathogenesis of anal
fissure, possibly by impairing tissue perfusion
and leading to ischemic ulcer (1, 2, 3 4). Conservative
management of the anal fissures traditionally
involves stool softeners, warm sitz baths and
the application of topical anesthetics. Chronic
fissures tend to be more resistant to conservative
management characterized by frequent recurrences
(5) . Surgical procedures to reduce resting anal
tone for the recalcitrant fissures are effective
but carry a significant risk of permanent minor
impairment of continence (6, 7). Manual anal dilatation
may cause irreversible, uncontrolled injury to
the internal and external anal sphincters (8)
with the associated incidence of fecal incontinence
being 39% (9). Lateral subcutaneous internal sphincterotomy
leads to successful healing of the fissure in
more than 90 % of patients but temporary incontinence
for the flatus or feces occurs in 0-30 % of the
patients (10). Such observations have fuelled
attempts to develop non-operative measures for
reducing internal sphincter spasm.
Nitric oxide has emerged as one of the most important
neurotransmitters mediating internal sphincter
relaxation. [10] Topical glyceryl trinitrate (GTN),
a nitric oxide donor produces a successful chemical
sphincterotomy and improves anodermal blood flow
[10]. The aim of this study was to present a more
pragmatic assessment of the ultimate usefulness
of GTN in the treatment of acute and chronic anal
fissures.
This is an uncontrolled
prospective clinical study
involving one hundred
and eight patients with
acute and chronic anal
fissure. Most of the patients
had tried traditional
conservative treatment
(such as ointments, suppositories
and laxatives) for long
duration, had presence
on examination of signs
of chronicity (skin tag
and or anal polyp), or
even previous surgical
intervention such as anal
dilatation with recurrence
of symptoms and signs,
but never used GTN. These
patients had full explanation
about chronic fissure
in ano including pathogenesis
and options of treatment,
mechanism of action and
side effects of GTN and
how to overcome or tolerate
them. These patients chose
to take this option as
the first choice instead
of other modalities such
as surgery or others.
Only pregnant and lactating
patients were excluded
from this treatment. All
patients above forty years
of age had barium enema
or colonoscopy during
their course of treatment.
The study was prospective,
and was done in Erbil
Teaching hospital, out
patient Department and
private clinic during
the period from June 2007
till August 2009. The
data was registered in
a pre-prepared form. This
form was filled in on
each visit (first time
GTN ointment was prescribed,
end of first week, end
of second week, and at
6th -8th week). Some did
come regularly for the
follow-up visits, others
did not. Those patients
who were not coming regularly
received phone calls to
be able to fill out the
forms. All patients had
a phone call to update
the data at the end of
the study period (i.e
August 2005). The follow
up period for all the
patients ranged between
4 months and 28 months.
All patients were evaluated
regarding pain, bleeding,
anal tone and fissure
healing. Patients who
stopped the treatment
were evaluated for the
cause. Patients who had
recurrence of symptoms
were evaluated regarding
the duration elapsed since
they finished their course
and the severity of the
recurrence and how it
was treated. Patients
who had severe recurrence
(i.e similar to the presenting
symptoms) were treated
with anal dilatation or
lateral sphincterotomy.
Glyceryl trinitrate 0.2%
ointment was prescribed
for three times per day
for 6-8 weeks. Few patients
extended their course
to 12 weeks which is acceptable
if needed according to
the latest international
literature. All patients
received in addition supportive
measures such as sitz
baths and fiber laxatives.
Drug preparation
Glyceryl trinirate 0.2%
ointment according to
the invention was prepared
by admixing 5 gm of 2%
by weight nitroglycerin
in white petrolatum, lanolin,
and distilled water with
45 gm white petrolatum
in a laboratory mixing
vessel at room temperature.
The resulting mixture
comprised 50 gm of a 0.2%
nitroglycerin ointment
(11).
Statistical analysis
Data were analyzed using
the Statistical Package
for Social Science (SPSS
version 15). The chi square
test of association was
used for categorical variables.
One-hundred and eight
patients took the GTN
0.2% ointment. Almost
all; 106 patients (98.1%)
were males. Age ranged
between 18-70 years
of age, and 50 patients
(46.3%) were between
30-49 years of age.
At presentation all
patients were complaining
of pain (100%), only
84 patients (77.8%)
had bleeding, and external
anal skin tag. Chronic
constipation was found
in 93 patients (86.1%).
Spastic colon was present
in 19 patients (17.6%).
Two patients had ulcerative
colitis disease. On
examination; all patients
(100%) had fissure,
104 patients (96.3%)
had anal spasm, and
86 patients (79.6%)
had skin tag. Almost
all, 106 patients (98.1%)
were treated conservatively,
and only 16 patients
(14.8 %) were treated
surgically before GTN
course. (Table 1)
Table 1: Symptoms
of acute and chronic
Fissure in 108 patients.

The response to treatment
was analyzed at first
week, second week, and
6th -8th week from the
start of the treatment.
Pain and bleeding showed
significant improvement
over the 6-8 weeks period.
By the sixth to eighth
week the pain was absent
in 55 patients (80.9%),
and was reduced in 8
patients (11.8 %). This
means 63 patients (92.7%)
showed good response
to GTN treatment. Bleeding
stopped in 72 patients
(83.7%), and was reduced
significantly in 6 patients
(7%). Total good response
was seen in 78 patients
(92.9%).(Tables 2, 3).
Table 2: History
of Pain in acute and
chronic fissure.
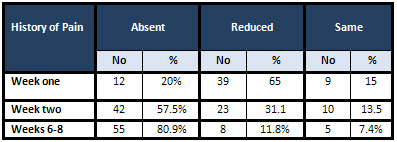
Pearson Chi-square:
50.5 (P<0.001
Table 3: History
of bleeding acute and
chronic fissure.
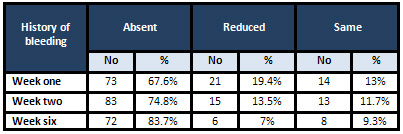
Pearson Chi-square:
7.64 (P<0.105
Regarding anal tone,
it became normal in
68 patients (80.5%)
and was spastic in 17
patients (20 %) at the
end of the treatment
course.(Table 4) Fissures
were also evaluated
regarding signs of healing,
where 80.3% were either
healed or showing signs
of healing. (Table 5).
Table 4: Anal tone
in acute and chronic
fissure of 108 patients.
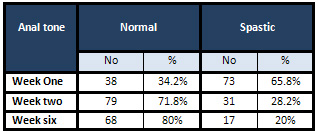
Pearson Chi-square:
51.44 (P<0.001)
Table 5: Healing
efficacy of GTN in 108
patients with acute
and chronic fissure.
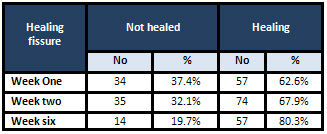
Pearson Chi-square:
6.003 (P<0.05)
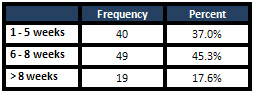
The duration of treatment
ranged between 1 week
and 28 weeks. Forty
nine patients took the
course for 6-8 weeks
(45.3%) and 19 patients
(17.6%) took the treatment
more than 8 weeks and
up to 20 weeks. (Table
6) This indicates that
68 patients (62.9%)
did not stop the treatment
and finished the course
within 6-8 weeks.
Table 6: Duration
of treatment with GTN
in 108 patients with
acute and chronic fissure.
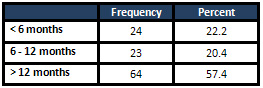
The duration of follow-up
was less than six months
in 24 patients (22.2%),
six to twelve months
in 23 patients (20.4%),
and more than 12 months
in 64 patients (57.4%).
This indicates that
almost half of our patients
had follow-up for more
than one year and more
than two-thirds for
6 to 12 months (Table
7).
Table 7: Duration
of follow-up in months
in 108 patients with
acute and chronic fissure
treated with GTN 0.2%
The patients who stopped
the GTN course early
(40 patients), had multifactorial
causes which were evaluated;
such as side effects
(mainly headache) in
25 patients (60%), noncompliance
to dose, frequency or
the drug finished before
the end of the course
in 39 patients (95%),
and patients who claim
no response to GTN course
were 21 patients (50%)
(Table 8).
Table 8: Causes of
stopping treatment with
GTN 0.2% in patients
with acute and Chronic
fissure

* The percent was calculated
from those who stopped
treatment (20 patients)
There were 47 patients
who had recurrence of
symptoms within six
months after finishing
or stopping the course.
The symptoms were either
mild or severe. There
was a significant strong
relationship between
recurrence of symptoms
and the duration of
treatment; the symptoms
recurred in a shorter
period if the treatment
was taken for a shorter
course, particularly
if it was taken for
less than a 6-8 weeks
period (Table 9).
The severity of recurrence
in these patients was
mild in 18 patients
(46.2%) and was treated
either with traditional
ointment or repeated
GTN course and was severe
in 29 patients (53.8%)
and was treated surgically
by anal dilatation.
Table 9: Treatment
of recurrence in relation
to severity
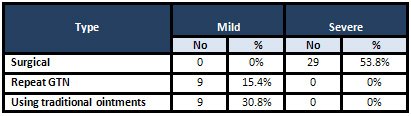
Pearson Chi-square:
47 (P<0.001)
The percent was calculated
from the patients who
had recurrence within
6 months (26 patients).
The present clinical
trial establishes the
clinical efficacy of
0.2% GTN ointment in
the treatment of anal
fissures. The published
data of a high cure
rate of 70-80% in various
studies [3,6] with a
paucity of significant
side effects are encouraging
Topical GTN ointment
is an effective alternative
to surgery in the treatment
of chronic fissure in
ano(8). Preparations
of 0.2% GTN ointment
is probably the most
widely used first line
treatment in the UK
with successful results
(3), but many patients
experience troublesome
headaches on this therapy.
The ointment is applied
2-3 times daily to the
distal anal canal for
up to 8weeks but in
some should be used
up to 12 weeks for the
fissure to heal.
In our study the chronic
fissure in ano was either
healed or healing in
80.3% in the 6-8 weeks
period. The healing
rate in 4-8 weeks course
in other studies was
71% with 0.5% concentration
(1), 67%, 65%, 62.5%,
and 84% with 0.2% concentration
(2, 3, 5,). There were
other studies which
showed no difference
in healing rates between
0.2% and higher concentrations
(6). Other studies have
also concluded that
two-thirds of their
patients will heal,
but over one-half will
develop headaches as
side effects of the
treatment (3). The headache
is usually mild, transient
and tolerable, often
diminishing in intensity
and duration with continued
application (3,6). In
some cases the headache
may be sufficiently
severe to reduce compliance
or lead to cessation
of treatment. One article
claimed that better
outcome was seen with
the use of higher concentration
(72% with 0.5% vs 64%
with 0.2%). (1) This
benefit, however, occurs
at the expense of more
headache and lower compliance
rate. In our study the
healing rate was high
with only 0.2% concentration
and non-compliance and
headache were studied
and found significantly
high in patients who
stopped their course
of treatment before
6-8 weeks. What remains
unclear in all published
series is whether headaches
are in part due to absorption
of GTN via the finger,
given that not all patients
use gloves while applying
the medication. Furthermore,
given the absence of
a reliable dosage system,
the actual quantity
may be different in
each patient.(1)
An uncontrolled prospective
observational study
looked at the use of
isosorbide dinitrate
spray in the treatment
of anal fissures.(2)
In 81patients studied,
symptoms had been present
for two to 120 months
with classical signs
of chronicity present
in only 61% of cases.
All the patients had
failed to heal after
three weeks of conservative
management. In this
group of patients, isosorbide
dinitrate 1.25 or 2.5
mg (one or two sprays)
applied three times
a day for four weeks
produced healing in
83% of patients at four
months. There was an
18% relapse rate after
a mean follow-up of
11 months, all of which
were successfully treated
with a further four
week course. Headaches
occurred in 19.5%.
In general, most studies
report healing in the
majority of cases within
eight weeks of treatment
(1, 3, 4 & 7). In
one article a review
through the Pub Med
(1996-May 2003) and
Cochrane Library (May
2003) for all reports
that compared non-surgical
therapy with surgery,
showed that GTN had
higher healing rates
than placebo (11 trials).
This also showed that
GTN had lower healing
rates than sphincterotomy
(4 trials) but did not
differ for minor incontinence.
GTN did not differ from
botulinum toxin injection
(botox) (2 trials) or
calcium channel blockers
(1 trial) (9).
The duration of treatment
in our patients ranged
between one week and
28 weeks. About 62.9%
took the treatment for
6-8 weeks or more.
Early recurrence (less
than 6 months) has occurred
in 48% of patients.
It does not appear to
be a problem as it was
mild in almost half
and was treated conservatively
either with traditional
ointments or repeated
GTN course. The recurrence
was severe in 29 patients
only and these were
the ones who needed
surgical treatment.
In our results we found
a significant strong
relationship between
the duration of treatment
and duration of recurrence.
This indicated that
prolonged courses of
treatment 8-12 weeks
or more had better results
and longer periods of
free of symptoms.
Other series showed
that fissures which
initially healed on
GTN will recur within
12 months but respond
to further courses of
GTN (6).
From our results and
other studies we conclude
that less than eight
weeks of treatment with
topical GTN is likely
to be unsuccessful in
truly chronic fissures
as it takes chronic
fissures eight weeks
to heal; indeed some
fissures may only partially
heal within eight weeks
but will fully heal
if treated longer (6).
The duration of follow-up
of our patients was
significantly high which
was not found in some
other studies. (1,2)
GTN is a useful therapeutic
modality in the management
of acute and chronic anal
fissures, with an 80.3%
healing rate in this study,
which are refractory to
dietary modifications,
fiber supplements and
sitz baths. As GTN is
safe and effective we
suggest performing a randomized
comparative study with
surgical gold standard
treatment.
1-
McCallion
K,
Review
article.
Progress
in
the
understanding
and
treatment
of
chronic
anal
fissure.
Postgraduate
Medical
Journal
2001;
77:753-758.
2-
Palazo
F.,
S.KAPUR,
Steward
M.
CullenT;
Glyceryl
trinitrate
treatment
of
chronic
fissure
in
ano:
One
year's
experience
with
0.5%
GTN
paste.
Journal
Royal
College
Surgeons
Edinburgh,
45
June
2000,
168-170.
3-
Jonas
M,
Scholefield
J.
Anal
fissure
and
chemical
sphincterotomy,
Recent
Advances
in
Surgery
24,
Chapter
9:
115-124.
4-
Kenny
S
E,
T
Irvine.
Double
blind
randomized
controlled
trial
of
topical
glyceryl
trinitrate
in
anal
fissure,
Arch
Disease
in
Child
2001;
85:404-407
5-
Carapeti
E
A,
Kamm
M.
Randomized
controlled
trial
shows
that
glyceryl
trinitrate
heals
anal
fissures,
higher
doses
are
not
more
effective,
and
there
is
a
high
recurrence
rate.
Gut
1999;
44:727-730
6-
Scholefield
J
H,
Bock
J
U.
A
dose
finding
study
with
0.1%,
0.2%,
and
0.4%
glyceryl
trinitrate
ointment
in
patients
with
chronic
anal
fissures.
Gut
2003;
52:
264-269.
7-
Mohender
M
Rajinish
M.
Randomized,
double-blind
trial
comparing
topical
nitroglycerine
with
xylocaine
and
proctosedyl
in
idiopathic
chronic
anal
fissure.
Indian
Journal
of
Gastroenterology;
2004,
volume:
23,
Issue:
3,
91-93.
8-Gupta
PJ.
Treatment
trends
in
anal
fissures
-
Topical
review.
Bratisal
Lek
Listy
2004;
105
(1):
30-34.
9-Nelson
R.
Review.
Medical
therapies
are
less
effective
than
surgery
for
anal
fissure,
Evidence
Based
Medicine
2004;
9:
112.
10-Altomare
DF.
Rinaldi
M;
Glyceryl
trinitrate
for
chronic
anal
fissure-
healing
or
headache?
Results
of
multicenter,
randomized,
placebo-controlled,
double-blind
trial.
Disease
of
Colon
Rectum
2000
Feb;
43(2):
174-9.
11-USP30-NF25
(United
States
Pharmacopia-National
Formulary).
Nitroglycerin
Ointment.
2009,
Page
2765
|
|
.................................................................................................................

|
| |
|
