|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor)
|
........................................................
|
|
Original Contribution
Perception and Parent’s
Knowledge about High Body Temperatures in Children
and Treatment Methods at Home
Saleh M. Alqahtani
[pdf]
DOI: 10.5742MEWFM.2019.93630
An investigation
into the outcomes of biliary atresia in Sulaimani,
Iraq
Adnan Mohammed Hasan, Mahdi Aziz Hama Marif,
Mohammed Fadhil Abbas
[pdf]
DOI: 10.5742MEWFM.2019.93631
Rheumatoid arthritis may be
one step further of systemic lupus erythematosus
Mehmet Rami Helvaci, Onder Tonyali, Mustafa
Yaprak, Abdulrazak Abyad, Lesley Pocock
[pdf]
DOI: 10.5742MEWFM.2019.93633
Mass Casualty Training
held on 2012 by Jordanian level 3 hospital-starbase,
UN Mission in Liberia, discussion and review
Mohammed Z. Alhasan, Ashraf (Mohammad SH.) A,
Odeh, Zuhier Ali A. Ikhwayleh,
Issam F. Alrbeihat, Ibrahim KH. Abuhussein
[pdf]
DOI: 10.5742MEWFM.2019.93632
Population and Community
Studies
Increased sexual
performance of sickle cell patients with Hydroxyurea
Mehmet Rami Helvaci, Onder Tonyali, Mustafa
Yaprak, Abdulrazak Abyad, Lesley Pocock
[pdf]
DOI: 10.5742MEWFM.2019.93634
|
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
AUSTRALIA
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| April 2019 - Volume
17, Issue 4 |
|
|
Perception and Parent’s
Knowledge about High Body Temperatures in Children
and Treatment Methods at Home
Saleh M. Alqahtani
Correspondence:
Dr. Saleh
M. Alqahtani,
Department of Child Health,
King Khalid University, Abha,
Kingdom of Saudi Arabia.
Email: salehalqahtani641@gmail.com;
smuadi@kku.edu.sa
Received: March 2019; Accepted: March 2019;
Published: April 1, 2019
Citation: Saleh M. Alqahtani. Perception and
Parent’s Knowledge about High Body Temperatures
in Children and Treatment Methods at Home. World
Family Medicine. 2019; 17(4): 4-10. DOI: 10.5742MEWFM.2019.93630
|
Abstract
Background: Fever
is one of the most common medical problems
in children that needs immediate medical
attention. The objective of the study
was to gauge the knowledge of parents
about fever in their children and what
treatment methods they do at home to treat
it through a questionnaire.
Patients and Methods: The
study involved random selection of Saudi
parents who have had febrile children.
Parents were interviewed using a standard
questionnaire to obtain sociodemographic
information and to assess their knowledge
about fever. The study also determined
methods that the parents were using at
home to treat fever.
Results:
A total of 353 parents completed the questionnaires.
The study sample consisted mainly of mothers
(62.3%). Most of the parents who participated
in the study have one child (47.3%) followed
by parents who have two children (42.8%).
There were only three parents who have
more than four children (.8%). Most of
the parents were between 18-30 years old
(46.7%) followed by parents between 31-40
years old (40.5%). There were only seven
parents who were older than fifty years
(2%). Most of the parents attained a college/university
degree (47.9%) followed by parents who
had secondary certificate (34.6%). Interestingly,
eight parents had a post graduate degree
(2.3%). Fifty four percent of the parents
are working (192) while the other forty
five percent are not (161). A total of
38% of the parents believed that the best
place to take the temperature of the child
is the ear (tympanic) followed by armpit
(axilla) 37.1%. The rest of the parents
took temperature orally (21%) and rectally
(4%) . In this study, about 43% believed
that 37 degrees Celsius is the normal
body temperature of a child followed by
36 degrees Celsius (20.4%). Approximately
30% of the parents considered a child
with a temperature of 38-38.4 degrees
Celsius as feverish followed by 38.5-39.90
degrees Celsius (26.3%).
In this study,
73.1% of the parents did not believe that
alternating drugs is useful in cases where
the temperature did not lower after administering
an antipyretic drug. Almost 50% of the
parents believed that seizure is the complication
of fever followed by brain damage, dehydration,
coma, and death. Parents’ most frequently
reported measurement of a child’s
temperature was best by using an electronic
thermometer (34.8%) followed by an ear
thermometer (28.3%). Other parents measured
the temperature of their child by using
their hands and with a mercurial thermometer.
Most parents measured the temperature
every 30 minutes to 1 hour (37.4%) followed
by every 15 to 30 minutes (23.2%). When
asked about the drug usually given to
the child to reduce fever, the majority
of the parents reported giving paracetamol
(80%) while the others gave antibiotics
(9.3%), ibuprofen (4.8%), and aspirin
(1.1%). We also found that most of the
parents use physical methods to relieve
and treat fever such as tepid sponge bath
with cold water (38.8%), cold showering
(24.9%), tepid sponge bath with hot water
(21.5%) and other methods. In order to
determine the right dose of the antipyretic
drug administered to the feverish child,
85% of the parents used a specific measuring
spoon or syringe containing the drug.
Others used a regular teaspoon or tablespoon.
Most of the
parents when asked how the right fever
lowering drugs and doses was decided,
they indicated that they would follow
the previous advice from the pediatrician
(43.6%, 39.4%). Others consulted a pharmacist,
or others, or relied on information gathered
from media.
Conclusions: This study shows that
parents should be more aware about high
body temperatures and its consequences.
There should be more health education
among parents to correct the misconceptions
they have about fever. Also, parents should
be informed about different home treatments
and their consequences. There is a need
to develop programs that educate parents
and provide them with information they
need to better address the fever of their
children.
Key words: Fever, Methods, High body
temperature
|
Our body temperature is controlled by the hypothalamus.
There are two types of signals being received
by the hypothalamus. These signals are assimilated
by the thermoregulatory center of the hypothalamus
to maintain normal temperature. The human metabolic
rate produces more heat than is necessary to
maintain the core body temperature in the range
of 36.5–37.5°C (97.7–99.5°F)
in a neutral temperature environment (1, 2).
Fever is defined as an elevation of the body
temperature above the normal variation. Normal
temperature in children is about 98.6°F
(37°C) when taken by mouth and 99.6°F
(37.5°C) when taken by anus. Many doctors
define a fever as an oral temperature above
99.5°F (37.5°C) or a rectal temperature
above 100.4°F (38°C).(3)
Body temperature measurement is most commonly
done to confirm the presence or absence of fever.
Many decisions concerning the investigation
of children are based on the results of the
temperature measurement alone. An incorrect
temperature measurement could result in delayed
detection of a serious illness or alternatively
an unnecessary infection.
A number of researchers published in the international
literature have reported that parents have different
conceptions, often erroneous, in relation to
the exact temperature values considered as fever
in childhood. Thus, concerns about fever are
composed of incorrect associations between the
peak of the fever and severity of the disease.
Concerns about fever by parents may be real
or imagined and therefore assessment and monitoring
of temperature is essential for decision making
at home and in hospital settings (4).
There are different methods in taking the temperature
of children. You can get the most accurate temperature
reading by taking their temperature rectally.
According to Harrison et al., rectal temperatures
are generally 0.4°C (0.7°F) higher than
oral readings. The lower oral readings are probably
attributable to mouth breathing, which is a
factor in patients with respiratory infections
and rapid breathing. Lower-esophageal temperatures
closely reflect core temperature. Tympanic membrane
thermometers measure radiant heat from the tympanic
membrane and nearby ear canal and display that
absolute value (unadjusted mode) or a value
automatically calculated from the absolute reading
on the basis of nomograms relating to the radiant
temperature measured to actual core temperatures
obtained in clinical studies (adjusted mode).
These measurements, although convenient, may
be more variable than directly determined oral
or rectal values. Studies in adults show that
readings are lower with unadjusted-mode than
with adjusted-mode tympanic membrane thermometers
and that unadjusted-mode tympanic membrane values
are 0.8°C (1.6°F) lower than rectal
temperatures.(2)
The study was made to assess the understanding
of the parents with children regarding high
body temperatures and to know the methods they
use at home as treatment aside from giving medications.
Demographic
Data
A
total
of
353
parents
completed
the
questionnaires.
The
distribution
of
the
socio-
demographic
characteristics
of
the
parents
who
participated
in
the
study
is
shown
in
Table
1.
Table
1:
Socio-demographic
data
of
parents
participating
in
the
study
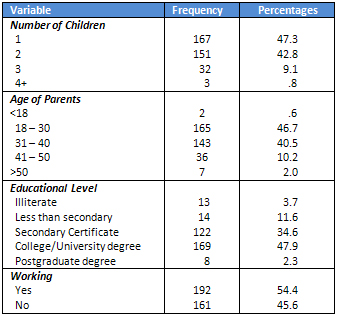
The
study
sample
consisted
mainly
of
mothers
(62.3%).
Most
of
the
parents
who
participated
in
the
study
have
one
child
(47.3%)
followed
by
parents
who
have
two
children
(42.8%).
There
are
only
three
parents
who
have
more
than
four
children
(.8%).
Most
of
the
parents
are
between
18-30
years
old
(46.7%)
followed
by
parents
between
31-40
years
old
(40.5%).
There
were
only
seven
parents
who
are
greater
than
fifty
years
old
(2%).
Most
of
the
parents
attained
a
college/university
degree
(47.9%)
followed
by
parents
who
had
secondary
certificate
(34.6%).
Interestingly,
eight
parents
had
post
graduate
degree
(2.3%).
Fifty
four
percent
of
the
parents
are
working
(192)
while
the
other
forty
five
percent
are
not
(161).
Parent’s
Beliefs
about
Fever
and
Its
Treatment
Table
2
shows
that
38%
of
the
parents
believed
that
the
best
place
to
take
the
temperature
of
child
is
the
ear
(tympanic)
followed
by
armpit
(axilla)
37.1%.
The
rest
of
the
parents
took
temperature
orally
(21%)
and
rectally
(4%)
respectively.
In
this
study,
about
43%
believed
that
37
degrees
Celsius
is
the
normal
body
temperature
of
a
child
followed
by
36
degrees
Celsius
(20.4%).
Approximately
30%
of
the
parents
considered
a
child
with
a
temperature
of
38-38.4
degrees
Celsius
as
feverish
followed
by
38.5-39.90
degrees
Celsius
(26.3%).
Table
2:
Beliefs
about
fever
and
its
treatment
as
reported
by
parents
(N=353)
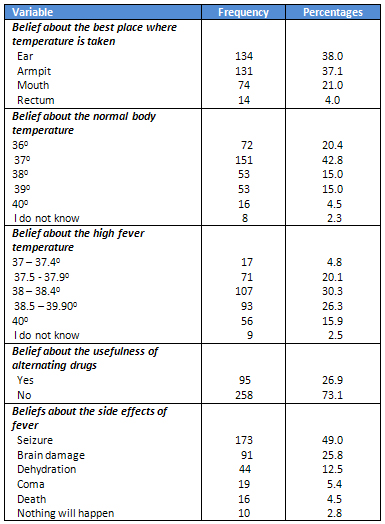
In
this
study,
73.1%
of
the
parents
did
not
believe
that
alternating
drugs
is
useful
in
cases
where
the
temperature
did
not
lower
after
administering
an
antipyretic
drug.
Almost
50%
of
the
parents
believed
that
seizure
is
the
complication
of
fever
followed
by
brain
damage,
dehydration,
coma,
and
death.
Parents’
Methods
in
Managing
Fever
As
shown
in
Table
3,
parents’
most
frequently
reported
measure
of
child’s
temperature
was
by
using
an
electronic
thermometer
(34.8%)
followed
by
an
ear
thermometer
(28.3%).
Other
parents
measured
the
temperature
of
their
child
by
using
their
hands
and
mercurial
thermometer.
Most
parents
measured
the
temperature
every
30
minutes
to
1
hour
(37.4%)
followed
by
every
15
to
30
minutes
(23.2%).
When
asked
about
the
drug
usually
given
to
the
child
to
reduce
fever,
the
majority
of
the
parents
reported
giving
Panadol/Fevadol
(80%)
while
the
others
gave
antibiotics
(9.3%),
ibuprofen
(4.8%),
and
aspirin
(1.1%).
We
also
found
that
most
of
the
parents
use
physical
methods
to
relieve
and
treat
fever
such
as
tepid
sponge
bath
with
cold
water
(38.8%),
cold
showering
(24.9%),
tepid
sponge
bath
with
hot
water
(21.5%)
and
others.
Table
3:
Parent’s
methods
in
managing
childhood
fever
(N=353)
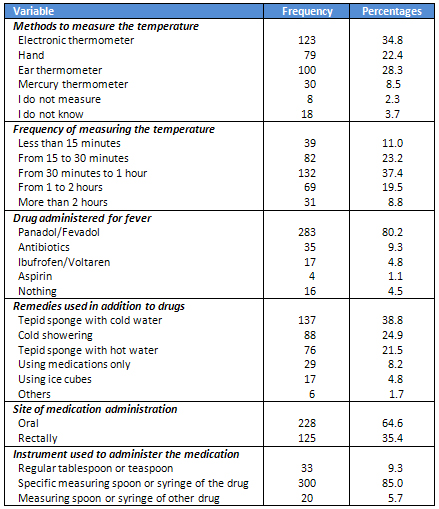
In
order
to
determine
the
right
dose
of
the
antipyretic
drug
administered
to
the
feverish
child,
85%
of
the
parents
used
a
specific
measuring
spoon
or
syringe
containing
the
drug.
Others
used
regular
teaspoon
or
tablespoon.
Parents’
Practices
in
Managing
Fever
Most
of
the
parents
when
asked
how
the
right
fever
lowering
drugs
and
doses
were
decided
indicated
that
they
would
follow
the
previous
advice
from
the
pediatrician
(43.6%,
39.4%).
Others
consulted
a
pharmacist,
consulted
others,
or
relied
on
information
gathered
from
media.
Predictors
of
Some
Practices
of
Fever
Management
Overall,
the
prevalence
of
administering
fever-lowering
medications
orally
among
this
study
sample
of
parents
was
63%
(Table
4).
The
route
used
to
administer
fever-lowering
drugs
was
found
to
be
significantly
associated
with
age,
gender,
and
number
of
children.
Click
here
for
Table
4:
Demographic
of
parents
by
route
of
administering
fever
lowering
medication
(N=353)
| | |
