|
Rheumatoid arthritis may be
one step further of systemic lupus erythematosus
Mehmet Rami Helvaci
(1)
Onder Tonyali (1)
Mustafa Yaprak (1)
Abdulrazak Abyad (2)
Lesley Pocock (3)
(1) Specialist of
Internal Medicine, MD
(2) Middle-East Academy for Medicine of Aging,
MD
(3) medi+WORLD International
Corresponding author:
Prof Dr Mehmet Rami Helvaci,
07400, Alanya, Turkey
Phone: 00-90-506-4708759
Email: mramihelvaci@hotmail.com
Received: February 2019; Accepted: March 2019;
Published: April 1, 2019
Citation: Helvaci M. et al. Rheumatoid arthritis
may be one step further of systemic lupus erythematosus.
World Family Medicine. 2019; 17(4): 17-20. DOI:
10.5742MEWFM.2019.93633
|
Abstract
Background: We
tried to understand whether or not there
are some relationships between rheumatoid
arthritis (RA) and systemic lupus erythematosus
(SLE) according to mean age of onset,
frequency, and gender distribution in
society.
Methods:
The study was performed in Medical Faculty
of the Mustafa Kemal University between
March 2007 and April 2016. All patients
applying to the Internal Medicine Policlinic
were included in the study.
Results: The
study included 223 males and 210 females,
totally. Their mean ages were 30.4 versus
30.3 years, respectively (p>0.05).
SLE was diagnosed in 6.0% of them (24
females and two males), and 92.3% of the
SLE patients were female. Mean age of
the SLE cases was 37.0 ± 13.6 (17-58)
years. On the other hand, RA was diagnosed
in 2.7% of them, so SLE was much more
frequent in society (p<0.001). Beside
that 50.0% of the RA patients were female
(six females and six males), so female
predominance of the SLE was higher than
RA (p<0.001). Mean age of the RA patients
was 44.5 ± 7.6 (30-57) years, so
RA patients were significantly older than
the SLE patients (p= 0.038).
Conclusion:
Because of the similar clinical presentation
types, similar treatment agents, similar
prognosis, and difficulties in differential
diagnosis, RA may be one step further
of the SLE due to its lower prevalence
in society (2.7% versus 6.0%, p<0.001),
similar prevalence in both genders (50.0%
versus 92.3% in females, p<0.001),
and higher mean age of onset (44.5 versus
37.0 years, p= 0.038).
Key words:
Rheumatoid arthritis, systemic lupus erythematosus,
chronic endothelial damage, atherosclerosis,
metabolic syndrome
|
Chronic endothelial damage may be the major
cause of aging and associated morbidity and
mortalities by causing tissue hypoxia and infarctions
all over the body. Much higher blood pressure
(BP) of the afferent vasculature may be the
major underlying cause, and probably whole afferent
vasculature including capillaries are mainly
involved in the process. Some of the well-known
accelerator factors of the inflammatory process
are physical inactivity, excess weight, smoking,
alcohol, chronic inflammation and infections,
and cancers for the development of irreversible
consequences including obesity, hypertension
(HT), diabetes mellitus (DM), cirrhosis, peripheric
artery disease (PAD), chronic obstructive pulmonary
disease (COPD), chronic renal disease (CRD),
coronary artery disease (CAD), mesenteric ischemia,
osteoporosis, and stroke, all of which terminate
with early aging and premature death. They were
researched under the title of metabolic syndrome
in the literature, extensively (1, 2). The syndrome
is characterized by a chronic low-grade inflammatory
process on vascular endothelium all over the
body (3, 4). The syndrome has become so common
all over the world, for example 50 million people
in the United States were affected (5). Physical
inactivity induced excess weight may be one
of the major underlying causes of the syndrome.
Excess weight is a disorder characterized by
increased mass of adipose tissue. The chronic
inflammation induced endothelial dysfunction
may be the action of excess weight for the increased
atherogenicity (6-9). Probably chronic vascular
endothelial inflammation including rheumatoid
arthritis (RA) and systemic lupus erythematosus
(SLE) may also accelerate the premature aging
process, and terminate with end-organ insufficiency
and premature death. We tried to understand
whether or not there are some relationships
between RA and SLE according to the mean age
of onset, frequency, and gender distribution
in society.
The study was performed in the Medical Faculty
of the Mustafa Kemal University between March
2007 and April 2016. All patients applying to
the Internal Medicine Polyclinic were included
into the study. Patients with a history of one
pack-year were accepted as smokers, and one
drink-year were accepted as drinkers. A complete
physical examination was performed by the same
internist. Cases with another inflammatory event
were treated at first, and the laboratory tests
and clinical measurements were performed on
the silent phase. A check up procedure including
serum iron, iron binding capacity, ferritin,
creatinine, hepatic function tests, markers
of hepatitis viruses A, B, C and human immunodeficiency
virus, a posterior-anterior chest X-ray film,
an electrocardiogram, a Doppler echocardiogram
both to evaluate cardiac walls and valves and
to measure systolic BP of pulmonary artery,
and an abdominal ultrasonography was performed.
Patients with RA were classified with the criteria
of early rheumatoid arthritis (ERA) (10). The
ERA criteria include a morning stiffness of
30 minutes or longer, arthritis of three or
more joint areas, arthritis of hand joints,
positivity of rheumatoid factor (RF), and positivity
of anti-cyclic citrullinated peptide antibody
(anti-CCP). RA is defined by the presence of
three or more of the criteria. SLE is classified
with the criteria of the American College of
Rheumatology of 1997 including discoid rash,
immunologic features, photosensitivity, neurologic
disorders (headache, depression, seizures, and
psychosis), oral ulcers, malar rash, arthritis,
serositis, hematologic disorders (leukopenia,
lymphopenia, thrombocytopenia, and hemolytic
anemia), antinuclear antibodies (ANA), and renal
involvement (proteinuria, low complement, red
blood cell casts, granular casts) (11). Four
of them are required for classification but
not for diagnosis. The criterion for diagnosis
of COPD is post-bronchodilator forced expiratory
volume in one second/forced vital capacity of
less than 70% (12). Systolic BP of the pulmonary
artery of 40 mmHg or higher is accepted as pulmonary
hypertension (13). CRD is diagnosed with a persistent
serum creatinine level of 1.3 mg/dL in males
and 1.2 mg/dL in females. Cirrhosis is diagnosed
with physical examination, liver function tests,
ultrasonographic evaluation, and tissue samples
in case of indication. An exercise electrocardiogram
is performed just in cases with an abnormal
electrocardiogram and/or angina pectoris. Coronary
angiography is taken just for the exercise electrocardiogram
positive cases. So CAD was diagnosed either
angiographically or with the Doppler echocardiographic
findings as the movement disorders in the cardiac
walls. Eventually prevalence, mean ages of onset,
and gender distributions of RA and SLE were
detected in society and compared in between.
Mann-Whitney U test, Independent-Samples t test,
and comparison of proportions were used as the
methods of statistical analyses.
The
study
included
223
males
and
210
females,
totally.
Their
mean
ages
were
30.4
versus
30.3
years,
respectively
(p>0.05).
SLE
was
diagnosed
in
6.0%
and
92.3%
of
the
SLE
patients
were
female
(24
females
and
two
males).
The
mean
age
of
SLE
cases
was
37.0
±
13.6
(17-58)
years.
On
the
other
hand,
RA
was
diagnosed
in
2.7%,
so
SLE
was
much
more
frequent
in
the
society
(p<0.001).
Beside
that
50.0%
of
the
RA
patients
were
female
(six
females
and
six
males),
so
female
predominance
of
the
SLE
was
higher
than
RA
(p<0.001).
The
mean
age
of
RA
patients
was
44.5
±
7.6
(30-57)
years,
so
the
RA
patients
were
significantly
older
than
the
SLE
patients
(p=
0.038)
(Table
1).
Table
1:
Characteristic
features
of
the
study
patients
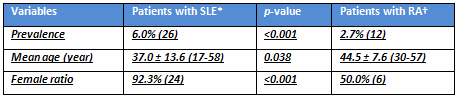
*Systemic
lupus
erythematosus
†Rheumatoid
arthritis
|

