|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
|
|
|
|
........................................................
|
Original
Contribution/Clinical Investigation
|
|
|
<-- Turkey -->
Very high
levels of C-reactive protein should alert the
clinician to the development of acute chest
syndrome in sickle cell patients
[pdf version]
Can Acipayam, Sadik Kaya, Mehmet Rami Helvaci,
Gül Ilhan, Gönül Oktay
<-- Jordan -->
Seroprevalence
of HBV, HCV, HIV and syphilis infections among
blood donors at Blood Bank of King Hussein Medical
Center: A 3 Year Study
[pdf
version]
Baheieh Al Abaddi, Maha Al Amr, Lamees Abasi,
Abeer Saleem, Nisreen Abu hazeem, Ahmd Marafi
|
|
........................................................ |
Medicine and Society
........................................................
International Health
Affairs
.......................................................
Education
and Training
.......................................................
Continuing
Medical Education
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| August 2014 -
Volume 12 Issue 6 |
|
Prevalence
of Helicobacter Pylori Infection in Adult Patients
with Dyspepsia in Gastrointestinal and Hepatology
Teaching Hospital, Baghdad 2012
Hadeer
Salah Al-Deen Abd Elwahhab (1)
Sanaa Jafar Hamodi Alkaisi (2)
Rayadh A. Zaydan (3)
(1) M. B. Ch. B postgraduate resident Doctor
in the Arab Board of Family medicine, Baghdad
.Iraq.
(2) M.B.Ch.B,F.I.B.M.S.\F.M Senior Specialist
Family Physician, Supervisor in the Residency
Program of Arab Board of Family Medicine, Member
in the Executive Committee of Iraqi Family Physicians
Society (IFPS), Co-manager of Bab Almudhum Specialized
Family Medicine Health Center, Baghdad, Iraq.
(3) C.A.B.M., F.I.C.M.S. (CE).Consultant
of Gastroenterology , Supervisor in the Residency
Program of Arab Board for Health Specializations
,in Subspecialty of Gastroenterology, Gastroenterology(GIT)
Center, Baghdad -Iraq.
Correspondence:
Dr.Sanaa Jafar Hamodi Alkaisi,
Co-manager of Bab Almudhum Specialized Family
Medicine Health Center,
Baghdad, Iraq.
Email:
drsanaaalkaisi@yahoo.com
|
Abstract
Background:
Dyspepsia is a common symptom with an
extensive differential diagnosis and a
heterogeneous pathophysiology. Helicobacter
pylori infection may be an etiological
factor in some patients. The infection
is chronic and common throughout the world,
with a higher prevalence in developing
than in developed countries.
Objectives: To demonstrate the
prevalence of Helicobacter Pylori infection
in adult patients with dyspepsia who underwent
upper Oesophagio-Gastro-Duodenoscopy so
early treatment can be made to prevent
it`s complications, and to estimate the
prevalence of positive endoscopic findings
in patients with dyspepsia.
Patients and methods: This is a
descriptive cross sectional study carried
out in the gastro-intestinal and hepatology
teaching hospital, Baghdad Medical City
during 2013 on data collected from reviewing
patient's files from the 1st of January
to 31st of December 2012 including all
adults 18 years and above of both sexes
with dyspeptic symptoms who were referred
for endoscopic evaluation of Helicobacter
Pylori infection by taking multiple
antral biopsies for histopathological
stain and evaluation of their endoscopic
findings.
Key words: helicobacter pylori,
adult patients, dyspepsia, Baghdad
|
Dyspepsia is a common symptom with an extensive
differential diagnosis and a heterogeneous pathophysiology.
It occurs in approximately 25 percent (range 13
to 40 percent) of the population each year, but
most affected people do not seek medical care.
[1]
Dyspepsia is often broadly defined as pain or
discomfort centered in the upper abdomen and may
include multiple and varying symptoms such as
epigastric pain, postprandial fullness, early
satiation (also called early satiety), anorexia,
belching, nausea and vomiting, upper abdominal
bloating, and even heartburn and regurgitation.
Patients with dyspepsia commonly report several
of these symptoms.[2]
The pathophysiology of functional dyspepsia is
poorly understood. However, researches have focused
on abnormal gastric motor function, increased
visceral sensitivity, psychosocial factors and
recently, Helicobacter pylori (H. pylori)
infection of the stomach. [3]
H. pylori infection is chronic and common
throughout the world, with a higher prevalence
in developing than in developed countries [4].
It has been reported that 20% to 60% of patients
with functional dyspepsia have evidence of
H. pylori gastritis and that eradication
of the organism results in symptomatic benefit
in a small number (10%) of these patients. Therefore,
patients younger than 55 years who have new-onset
dyspepsia without alarm features should undergo
H. pylori testing and treatment if infection
is confirmed. [5]
H. pylori infection can be diagnosed
by non-invasive methods or by endoscopic biopsy
of the gastric mucosa. The non-invasive methods
include the urea breath test, serologic tests
and stool antigen assays. Histology of endoscopically
taken biopsy has a very high sensitivity and
specificity of 96% and 98.8% respectively, even
though it requires expertise for interpretation.
[6]
Although there are several reports on the correlation
between H. pylori infection and clinical
outcomes, the results remain unclear and show
discrepancies. [7] This study therefore determined
to investigate H. pylori infection and its relation
with dyspepsia.
1. To estimate the prevalence of H.
Pylori infection in adult patients with dyspepsia
who underwent upper Oesophagio-Gastro-Duodenoscopy
(OGD) by histopathological stain so early treatment
can be made to prevent it`s complications.
2. To estimate the prevalence of positive
endoscopic findings in patients with dyspepsia.
Study Design: This is a descriptive cross
sectional study carried out in the GIT and hepatology
teaching hospital, Baghdad-Medical City during
2013 on data collected from reviewing patient's
files from the 1st of January to 31st of December
2012.
Inclusion criteria: Any patient more than
18 years old of both sexes who presented to the
GIT hospital during the year 2012 with any of
the dyspeptic symptoms and was diagnosed as having
dyspepsia according to Rome III and admitted for
endoscopic evaluation of H. Pylori infection
by taking multiple gastric biopsies for histopathological
stain and evaluation of their endoscopic findings
was included.
Exclusion criteria: None of the patients
selected were on antibiotic treatment for the
last 4 weeks before endoscopy, and none was on
NSAID's or PPI or steroids therapy, and none of
them had hematemesis or melena at presentation.
Data collection: Data was collected from
patients file information in regard to patient's
name, age, gender, residency and presenting symptoms
(postprandial fullness, early satiation, epigastric
pain, epigastric burning, bloating, nausea, vomiting
and belching), endoscopic findings and histopathological
stain results for H. Pylori. Data was collected
during a three months period from the 1st of January
to 31st of March 2013, on a basis of one day per
week.
Endoscopy: Upper gastroendoscopy by
video-endoscope was performed on each patient
for the evaluation of gastro-duodenal changes
and biopsy collection. Patients were fasted
overnight. The esophagus, stomach and duodenum
were all visualized and mucosal findings on
endoscopy were noticed. Three antral biopsies
were obtained for histology.
Histology: Biopsies were placed in 10%
formalin and then processed for histological
examination. Sections were stained with Hematoxylin
and Eosin stain (H & E stain) and examined
by an experienced histopathologist.
Limitations of the study:
The main limitations found for this study were:
1. This is a cross sectional study so
temporal relationship between cause-effect cannot
be determined.
2. Shortage of information available
on the patients in the hospital records.
Statistical analysis: Data of all patients
were checked for any errors or inconsistency
then transferred into computerized statistical
software; Statistical Package for Social Sciences
(SPSS) version 17 was used in all statistical
analysis and procedures. The student t test
was used to find the significance of differences
in mean age in patients with and without H.
Pylori infection. Chi square (X2)
was used to find the significance of differences
in the distribution of H. Pylori infection
among patients according to different variables
in the study and to assess the significance
of the relation between H. Pylori infection
and these variables. Fisher's exact test was
used alternatively when the chi square was inapplicable.
The level of significance was set at P-value
< 0.05
to be considered as a statistically significant
difference.
H. Pylori infection was detected in
164 (82%) patients versus 36 (18%) patients
who were free of H. Pylori infection.
The relation of H. Pylori infection with
age from different aspects of view: There was
a statistically significant relation between
age and the prevalence of H. Pylori infection,
(P-value =0.001); the infection was more prevalent
among patients with age (28 - 37) years followed
by those aged <
27 years. None of those aged >
78 years had positive H. Pylori infection,
(Table 1).

Table 1: Relation between H. Pylori infection
and age of the patient
H. Pylori infection was present in 93
(78.2%) of 119 males and 71 (87.7%) of 81 females
with no statistically significant difference
between both genders in the prevalence of H.
Pylori infection, P-value >0.05, (Table 2).
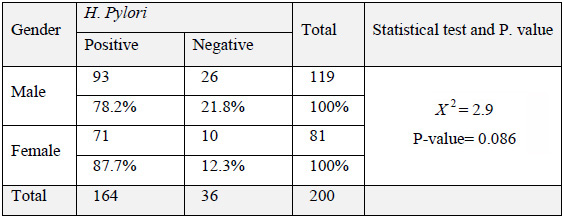
Table 2: Relation between H. Pylori infection
and gender
H. Pylori infection was more prevalent
among patients from Salah-Aldeen province (100%),
while there was none among patients of Basra
province (0.0%), P-value = 0.038, (Table 3).
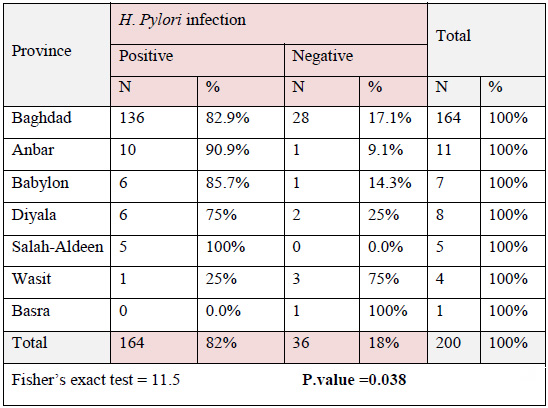
Table 3: Relation between H. Pylori infection
and provinces of residency
Summarization of the distribution of symptoms
according to the presence of H. pylori
infection and multiple complaints were recorded
in the same patient. There was no statistically
significant relation between symptoms and H.
Pylori infection, P-value >0.05, (Table
4).
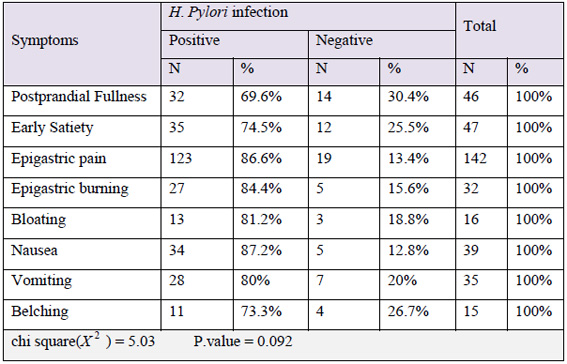
Table 4: Relation between H. Pylori infection
and symptoms
The infection rates in patients with D.U. and
hiatus hernia were significantly higher than
the rates among patients with other endoscopic
finding or with normal endoscopic findings;
P. value was highly significant (<0.001)
( Table 5).
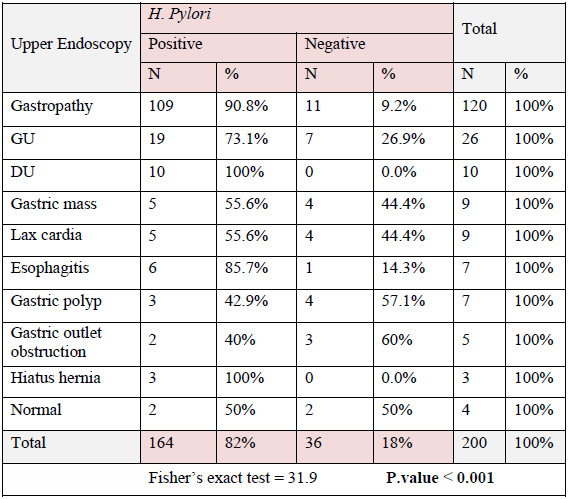
Table 5: Relation between H. Pylori infection
and endoscopic findings
This study shows the relation between dyspeptic
symptoms, endoscopic findings and various patient`s
parameters with H. Pylori infection among
the study sample.
Overall H. Pylori infection presents in
82% of the study sample where 18% were free of
the infection. This agrees with studies done in
Iraq (Mosul[8], Anbar[9], Basra[10]), Saudia Arabia
[11], North Jordan [12], Iran [13] , Kuwait [14],
and Libya [15].
Whereas a lower rate of infection was detected
in Jammu/ India[16], Jammica / Italy[3], Thailand[7].
The higher rate of detection of H. pylori in this
study and other developing countries of the Eastern
Mediterranean Region than in developed countries
may be attributed to the genetic predisposition
of the ethnic groups (mainly Arabs) or to local
environmental issues, including dietary factors,
inadequate living conditions, poor sanitation,
hygiene and overcrowding.
Prevalence rates of H. pylori infection
had shown a strong relation with young age group,
residency of middle provinces of Iraq, positive
endoscopic findings, but not with gender or presenting
symptoms. It had been significantly found that
the prevalence of H. Pylori infection decreased
with advancing age (P-value = 0.001) as it is
acquired at younger age. This is in accordance
to the results on Saudi patients [11], Iran [13],
Libya [15], Jammu/ India [16]. While in North
Jordan [12] the prevalence of H. Pylori
increases significantly with age (100% infection
rate in patients over 80 years of age). This was
more proven when comparing the mean age for patients
with positive and negative H. Pylori infection.
Where the mean age for patients with positive
H. Pylori infection was younger than that
of those free of it (40.16 ± 15.5 vs.51.1
± 18.7) years respectively and this difference
was statistically significant, P-value =0.002.
This may indicates that the infection with H.
Pylori occurs at earlier age. Factors such
as severe atrophy or intestinal metaplasia mean
that the local environment is no longer ideal
for the growth of H. pylori. This may contribute
to the lower prevalence in elderly patients.[13]
Males were more infected than females, and the
prevalence of H. Pylori infection among
males was less than that among females involved
in the study (78.2% vs 87.7%) with no statistical
significant relation (P- value = 0.086). The same
results were found in Anbar/ Iraq [9], Saudia
Arabia [11], Jammu/ India [16].
While in North Jordan [12], Kuwait [14] females
were more infected than males with lower infection
rate among females than males but also with no
statistical significant relation.
H. Pylori was strongly related to provinces
of residency (P- value =0.038), and it was most
prevalent among patients from provinces in the
middle of Iraq,while the least infection rate
was found in patients from provinces in the South.
This difference may be because of the small sample
size or may be related to different living standards
including overcrowding and atmosphere temperature.
Epigastric pain was the most frequent symptom
seen in 75% of patients with positive H. pylori
infection while belching being the least frequent
one. This result agrees with the results of Iran
[13], Jammu/ India[16] and Jamica/ Italy [3].
This may be explained in that epigastric pain
especially if associated with dyspeptic symptoms
is more associated with abnormal gastric pathology.[11]
On the other hand H. Pylori infection was
most prevalent in patients suffering from nausea
and least prevalent in patients with postprandial
fullness; but the prevalence of H. Pylori
infection has no statistical significant relation
with the presenting symptom in this study. It
is now accepted that H. pylori is not associated
with a specific symptom profile. This was like
North Jordan [12]. While in Saudi Arabia[11] and
Iran [13] H. Pylori infection was more common
among patients suffering from epigastric pain.
The most common +ve endoscopic finding in this
study was gastropathy in 120 patient (60%) and
the least was Hiatal Hernia (3 patients). There
was a significant relation between H. Pylori
infection and endoscopic findings (p-value <
0.001). It was seen in all patients with D.U.
and hiatal hernia (100% for each). While in Mosul/
Iraq [8], North Jordan[12] and Libya[15] infection
rate was 100% among patients with G.U. The possible
explanation for the lower infection rate among
patients of this study with G.U. than the other
studies is that it may be due to errors in the
sampling technique. One half of the patients of
this study with normal endoscopic findings have
+ve H. Pylori. This goes with results from
Libya [15], Thailand [7] and differs from Jamaica/
Italy [3], and this may indicate that H. Pylori
may be a cause of functional dyspepsia.
The H. pylori infection is frequent in
patients with dyspepsia which decreases with increasing
age with higher infection rates in patients from
provinces of the middle of Iraq. Positive endoscopic
findings were significantly related to H. pylori
infection and pathological dyspepsia has higher
infection rate than NUD. Although half of the
patients with NUD were reported to harbor H.
pylori infection, yet this study cannot prove
a causality relationship between H. Pylori
infection and dyspepsia because the descriptive
study cannot prove it.
1. There is a need to increase awareness
of the role of H. Pylori in causation
of dyspepsia.
2. There is a need for early detection
of H. pylori infection and its eradication to
prevent medication abuse of acid suppression
and an improvement in overall quality and severity
of dyspeptic symptoms.
3. There is a need for more rapid and
non-invasive methods for screening of H.
Pylori infection in patients with un-investigated
dyspepsia to be available at the primary care
centers (as a cost effective methods) to reduce
the overcrowding on specialty hospitals and
minimizes cost and consequences of delayed treatment
because dyspepsia is common and strongly correlated
to H. Pylori infection.
4. It is recommended that endoscopy be
used for patients with dyspepsia that is undiagnosed
by other methods and unresponsive to treatment
to identify those who are infected by H.
pylori and treated accordingly.
5. It is recommended to do analytic study
to prove the cause and effect relationship which
include therapeutic interventional studies to
prove the improvement of symptoms after treatment.
1- Longstreth GF, Talley
NJ, Grover S. Functional
dyspepsia. UpToDate[CD-Room].
2011; 19(3).
2-Tac J. Dyspepsia. In:
Feldman M, Friedman LS,
Brandt LJ, editors. Sleisenger
and Fordtran's gastrointestinal
and liver disease: pathophysiology,
diagnosis, management.
9th ed. Saunders: Elsevier;
2010. P. 183-193.
3-Lee MG, Emery H, Whittle
D, Jackson D, Donaldson
EK: Helicobacter pylori
infection in patients
with functional dyspepsia
in Jamaica. The Internet
Journal of Tropical Medicine.
2009[cited 2012 Oct 19];
5(2): [about 3 p.]. Available
from: http://www.ispub.com/journal/the-internet-journal-of-tropical-medicine/volume-5-number-2/
4-Siddiqui ST, Naz E,
Danish F, Mirza T, Aziz
S, Ali A. Frequency of
Helicobacter pylori in
biopsy proven gastritis
and its association with
lymphoid follicle formation.
J Pak Med Assoc. 2011;
61(2): 138-141.
5-Herrine SK, Fekete T,
Bosworth BP, Kozuch P,
Loren DE, Navarro VJ,
et al. Gastroenterology
and hepatology. In: Alguire
PC, editors. MKSAP15 [CD
Room]. USA: American College
of physicians; 2009.
6-Mustapha SK, Bolori
MT, Ajayi NA, Nggada HA,
Pindiga UH, Gashau W,
et al. Endoscopic findings
and the frequency of Helicobacter
Pylori among dyspeptic
patients in north-eastern
Nigeria. The Internet
Journal of Gastroenterology.
2007 [cited 2012 Oct 19];
6(1): [about 4 p.]. Available
from: http://www.ispub.com/journal/the-internet-journal-of-gastroenterology/volume-6-number-1/
7-Chomvarin C, Kulsuntiwong
P, Mairiang P, Sangchan
A, Kulabkhow C, Chau-in
S, et al. Detection of
H. Pylori in dyspeptic
patients and correlation
with clinical outcomes.
Southeast Asian J Trop
Med Public Health. 2005;
36(4): 917-922.
8- Ayoub MA. Frequency
of Helicobacter Pylori
infection among dyspeptic
patients in Mosul. A dissertation
submitted to Iraqi Board
for Medical Specializations
in Medicine. 2009.
9- Baqir HI, Abdullah
AM, Al-Bana AS, Al-Aubaidi
HM. Sero-prevalence of
Helicobacter Pylori infection
in unselected adult population
in Iraq. IJGE. 2002; 1(3):
22-29.
10- Al-Sulami A, Al-Kiat
HS, Bakker LK, Hunoon
H. Primary isolation and
detection of Helicobacter
Pylori from dyspeptic
patients: a simple, rapid
method. Eastern Mediterranean
Health Journal. 2008;
14(2): 168-176.
11- Abo-Shai MA, El-Shazly
TA, Al-Johani MS. Clinical,
endoscopic, pathological
and serological findings
of Helicobacter Pylori
infection in Saudi patients
with upper gastrointestinal
diseases. British Journal
of Medicine and Medical
Research. 2013; 3(4):
1109-1124.
12- Bani-Hani KE, Hammouri
SM. Prevalence of Helicobacter
Pylori in north Jordan.
Endoscopy based study.
Saudi Med J. 2001 Oct
[cited 2014 April 14];
22 (10): 843-7. Available
from: http://www.ncbi.nlm.nih.gov/pubmed/?term=Prevalence+of+Helicobacter+pylori+in+Northern+Jordan.+Endoscopy+based+study.
13- Shokrzadeh L, Baghaei
K, Yamaoka Y, Shiota S,
Mirsattari D, Porhoseingholi
A, et al. Prevalence of
Helicobacter Pylori in
dyspeptic patients in
Iran. Gasroenterology
Insights. 2012; 4(8):
24-27.
14- Abahussain EA, Hasan
FAM, Nicholls PJ. Dyspepsia
and Helicobacter Pylori
infection: analysis of
200 Kuwaiti patients referred
for endoscopy. Annals
of Saudi Medicine. 1998;
18(6): 502-505.
15- Bakka AS, El-Gariani
AB, AbouGhrara FM, Salih
BA. Frequency of Helicobacter
Pylori infection in dyspeptic
patients in Libya. Saudi
Med J. 2002; 23(10): 1261-1265.
16- Kumar R, Bano G, Sharma
S, Gupta Y. Clinical profile
in H. Pylori positive
patients in Jammu. JK
Science. 2006; 8(3): 148-150.
|
|
.................................................................................................................

|
| |
|
