|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
|
|
|
|
........................................................
|
Original
Contribution/Clinical Investigation
|
|
|
<-- Saudi Arabia -->
Academic Leadership
Development (ALD) Program at College of Medicine,
Jeddah; King Saud bin Abdulaziz University for
Health Sciences
[pdf version]
Saad Abdulrahman Alghmdi, Wesam Abuznadah, Almoutaz
Alkhier Ahmed
<-- Iraq -->
A new method in the management
of wrist ganglion (Silk thread passed through
the ganglion); in comparison with other traditional
methods
[pdf version]
Abdulqadir M. Zangana, Kawa F. Dizaye
<-- Egypt-->
Seroprevalence
of Measles, Rubella, Mumps and Varicella Specific
Antibodies in Primary School Children
[pdf version]
Reda Sanad Arafa, Ghada Saad Abdelmotaleb, Raneyah
Hamdy Mahmoud Shaker,
Inas Abdulmonem Elsayed, Rabab Fawzy Salim Baioumy,
Nesreen Mohamad Zain El Dean, Lamyaa Hussain
Abdulrahman Seliem
|
|
........................................................ |
Medicine
and Society
........................................................
Clinical
Research and Methods
........................................................
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| January 2016 -
Volume 14, Issue 1 |
|
|
A new method in the management
of wrist ganglion (Silk thread passed through
the ganglion); in comparison with other traditional
methods
Abdulqadir M. Zangana
(1)
Kawa F. Dizaye (2)
(1) Professor of Surgery, CABS-FICS-MD, Head
of Department of surgery, Consultant Surgeon,
College of Medicine, Hawler Medical University,
Iraq.
(2) Professor of Pharmacology, HD, MSc, PhD,
Head of department of Pharmacology College of
Medicine, Hawler Medical University, Iraq.
Correspondence:
Dr. Kawa Dizaye
Professor of Pharmacology, HD, MSc, PhD,
Head of department of Pharmacology College of
Medicine,
Hawler Medical University, Iraq.
Tel: 009647504452392
Email: doctorkawa@gmail.com
|
Abstract
Objectives:
To compare a new method of ganglion management,
efficacy of resolution, frequency of complications
and recurrence of managing dorsal wrist
ganglions with aspiration followed by
intra-cystic injection of Methylprednisolone
and surgical excision and our new procedure
Silk thread passed through the ganglion.
Study Design : A
prospective descriptive study.
Place and Duration of Study: This
is a prospective study conducted at the
Department of Surgery Erbil Teaching Hospital-Erbil,
Kurdistan Region of Iraq from April 2005
to June 2014.
Patients and Methods:
A total of 785 patients were included
in this study,120 cases were excluded
from the study because they were lost
to follow-up. All patients were thoroughly
examined to exclude the other causes of
wrist swelling. The patients were divided
into three groups A, B &C according
to their choice of treatment. Group A
were treated by surgical excision, Group
B were treated by aspiration followed
by steroid injection and group C by Silk
thread passed through the ganglion. Baseline
Data were recorded preoperatively and
postoperative data were obtained at the
intervals of 2 weeks, 6 weeks, 3 months,
and 6 months. At the end of 6 months the
data form was completed and results analyzed.
Results: Patient's
satisfaction was higher in Group C after
Silk thread passed through the ganglion
followed by surgical excision even if
the ganglions recurred. The recurrence
rate was 4 % in Silk thread passed and
24% surgical excision group and 43% in
aspiration with steroid injection in group
B.
Conclusion:
In this study Silk thread passed through
the ganglion had better results compared
to surgical excision and to aspiration
and injection of Methylprednisolone.
Key words: Dorsal,
Wrist Ganglion, Silk thread passed through
the ganglion, surgical excision, aspiration,
Methylprednisolone injection.
|
Ganglia are the most common benign soft tissue
tumors of the hand. They represent 50% to 70%
of all soft tissue tumors of the hand, and in
some series, the percentage is even higher (1).
These soft murine-filled cysts are usually attached
to the adjacent underlying joint capsule or
tendon sheath (2).
The cyst expands in size and the fluid cannot
flow freely back into the synovial cavity. Dorsal
wrist represents 70% of all ganglion and volar
writ ganglion up to 20 %.(3)
Dorsal ganglion cyst originates from the scapholunate
joint, often with direct attachment to the scapholunate
interosseous ligament (ISLIL) (4).
The ganglions usually appear spontaneously without
any particular cause; pain associated is dull
aching pain and severity is not related to the
size of ganglions. The diagnosis of the ordinary
wrist ganglion should rarely be in doubt when
the mass is in typical site and has the usual
size, shape and consistency, though other serious
entities may simulate wrist ganglion (5).
Different treatment modalities for wrist ganglions
have been described in literature ranging from
observation reassurance, digital pressure rupture
with mallet, aspiration with or without different
agents, subcutaneous tenetomy dissection and
cross fixation with heavy sutures to orthoscopic
resection and surgical excision (6).
Surgical excision of wrist ganglia has been
reported to have the best success rates in terms
of recurrence; for example Angelides and Wallace
in1976 reported a 99% success rate (7). However,
the treatment is relatively expensive and can
only be offered reliably in a specialist hand
center. The complications associated with the
treatment by surgical excision are recurrence,
infection, wound healing, neuromas, joint stiffness
and decreased grip strength. Aspiration and
injection of steroid has higher recurrence rate,
but other complications are much lower than
that of surgical excision (8).
This prospective study was conducted to find
out whether aspiration and injection of ganglion
with Methylprednisolone was effective as surgical
excision and Silk thread passed in a cross manner.
Seven
hundred
and
eighty
five
patients
were
included
from
the
outpatient
department
of
surgery
Erbil
Teaching
Hospital,
Erbil,
Kurdistan
Region
of
Iraq
from
April
2005
to
June
2014.
All
patients
were
thoroughly
examined
by
the
attending
physician
to
exclude
the
other
causes
of
dorsal
wrist
swelling.
All
785
patients
were
informed
about
the
three
treatment
modalities
and
they
were
divided
into
three
groups
A,
B
and
C
according
to
their
options.
Group
A
comprised
163
patients
treated
by
surgical
excision
and
155
formed
Group
B
and
were
dealt
with
by
aspiration
and
Methylprednisolone:
20-40
mg
injections
and
464
formed
Group
C
dealt
with
Silk
thread
passed
in
a
cross
manner
(Figure
1).
There
was
no
sex
or
age
limit.
Those
patients
who
were
operated
on
or
aspirated
in
the
past
were
excluded
from
this
study.
Blood
test
including
blood
CP,
ESR,
RA
factor
and
X-Rays
wrist
joint
AP
and
Lateral
view
were
performed
in
all
cases.
In
Group
A
surgical
excision
was
performed
under
General
Anaesthesia.
Pneumatic
tourniquet
was
applied
in
most
cases.
The
incision
used
respected
the
skin
creases
and
was
long
enough
to
give
satisfactory
exposure
of
the
skin
lesion.
Attempt
was
made
to
exercise
a
generous
capsular
margin
about
its
base
and
joint
capsule
was
left
open
and
cauterized.
One
shot
of
I.V
3rd
generation
Cephalosporin
was
given
at
time
of
induction
followed
by
3
doses
of
oral
antibiotics
postoperatively.
Prior
to
wound
closure
tourniquet
was
released,
hemostasis
secured
and
the
wound
was
closed
with
prolene.
Patients
were
called
for
follow
up
on
the
2nd
week,
6th
week,
and
3,6
month;
findings
were
documented.
The
patients
in
Group
B
and
C
were
in
OPD
in
supine
position
with
wrist
flexed
on
a
towel.
The
area
was
prepared
and
draped.
Syringe
(10ml)
with
18
gauge
needle
was
inserted
in
the
center
of
the
ganglion;
gelatinous
content
was
aspirated
and
demonstrated
to
the
patient.
Syringe
was
removed
leaving
needle
in
place.
1.5ml
local
anesthetic
injection
Xylocaine
and
40
mg
of
methylprednisolone
was
injected.
In
group
C,
no.1
silk
on
cutting
needle
was
inserted
in
the
ganglion
horizontally
from
side
to
side;
a
ring
of
silk
created
gelatinous
content
was
evacuated
by
gentle
digital
pressure
on
the
ganglion
xylocaine
lubricant
was
applied
on
the
silk
ring
and
the
patient
advised
to
rotate
the
silk
ring
and
apply
gentle
digital
pressure
on
the
ganglion
3
times\day
for
7
days
.
Patients
were
asked
to
follow
up
at
the
OPD
and
2
weeks,
6
weeks,
and
6
months
findings
were
documented
and
results
were
analyzed.
Technique
of
new
in
cross
manner:
Under
aseptic
measures,
a
silk
No.1
on
a
curved
needle
passed
through
the
ganglion
(Figure
1)
and
aspiration
of
the
jelly
like
transparent
material
was
performed
by
applying
pressure
on
the
ganglion
with
the
thumb
jelly
material
comes
out
at
both
sides
of
the
needle
puncture
and
silk
fixed
as
a
Ring.
After
complete
evacuation
a
crepe
bandaging
was
applied
over
the
wrist
(Figures
1,
2,
3,
4
)
On
the
second
day
after
procedure
the
first
dressing
was
removed
and
patients
start
to
rotate
the
silk
in
both
directions
with
applying
local
digital
pressure
and
antibiotic
ointment.
Silk
was
removed
on
the
12th
day.
In
this
procedure
no
anesthesia
was
used
during
the
procedure
all
patients
were
followed
up
every
month
for
an
initial
3
months
and
at
6
months
interval
for
one
year.
Figure
1:
dorsal
wrist
ganglion
classical
site

Figure
2:
Insertion
of
needle
through
the
ganglion
after
application
of
topical
anesthesia
under
aseptic
condition

Figure
3:
Farther
advancement
in
the
process
of
needle
insertion
creating
a
ring
in
the
silk

Figure
4:
The
procedure
has
been
completed

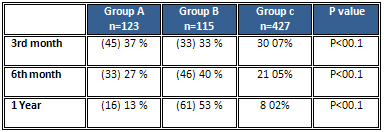
Table
1:
Resolution
of
pain
at
different
intervals

Table
2:
Wrist
stiffness
in
both
groups
at
different
intervals
During
the
study
period
from
April
2005
to
June
2014,785
patients
with
dorsal
wrist
ganglion
were
included
in
this
study
532
patients
were
female
and
253
were
male.
Patient's
age
ranged
from
18-38
years,
mean
age
was
25
years.
In
this
study
120
patients
were
lost
during
follow
up
leaving
665
patients.
One
hundred
and
twenty
three
patients
in
group
A
,
115
patients
in
group
B
and
427
in
group
C
were
available
for
follow
up
at
6
month.
Complete
resolution
of
pain
in
group
A,
B
&
group
C
at
different
follow
up
intervals
are
shown
in
Table
1.
Stiffness
of
wrist
was
observed
in
all
3
groups
which
improved
at
different
intervals
in
group
A.
In
group
B
stiffness
increased
in
late
follow
up
probably
because
of
more
recurrence
and
completely
improved
in
the
first
month
shown
in
Table
2.
At
the
end
of
six
month
recurrence
rate
was
24%
(29
patients)
in
group
A
as
compared
to
group
B
where
43
%
(49
patients)
presented
with
recurrence
while
recurrence
rate
in
group
C
was
4%(17)
.
There
were
four
cases
of
superficial
infection
in
group
A
which
responded
to
antibiotics
and
dressing.
There
was
one
case
of
change
in
skin
color
in
group
B,
and
8
cases
with
superficial
infection
in
group
C.
A
ganglion
in
a
musculoskeletal
system
is
spherical
accumulation
of
fluid
produced
from
an
adjacent
joint
capsule
or
tendon
sheath.
It's
not
a
neoplasm
because
it
is
a
cellular,
and
it's
not
a
cyst
because
the
collection
of
clear
viscous
fluid
is
contained
in
the
cavity,
which
is
not
lined
by
epithelium(1).
Dorsal
wrist
ganglion
is
the
most
common
non-tumorous
swelling
of
the
wrist
(2,
5,
6).
This
prospective
clinical
trial
compared
the
treatment
of
ganglion
by
either
aspiration
and
steroid
injection
or
surgical
excision
and
Silk
thread
passed
through
the
ganglion.
Different
treatment
methods
for
wrist
ganglion
are
reassurance,
rupture,
and
aspiration
with
or
without
different
agents,
surgical
excision
and
arthroscopic
resection
(7,
9).
Explanation
of
the
benign
nature
of
ganglion
and
natural
history
that
it
may
fluctuate
in
size
over
time
can
relieve
the
fear
of
malignancy
(10).
Results
of
different
treatment
methods
reported
literature
are
variable.
There
is
general
impression
that
Silk
thread
passed
in
through
the
ganglion
offers
excellent
result
comparing
with
open
excision
and
aspiration
with
or
without
different
agents,
probably
on
the
basis
of
Angelides
and
Wallace's
(2006)
study
reporting
1
%
recurrence
rating
(11)
Clay
and
Clement
(2008)
have
also
shown
low
recurrence
rate
of
3
%
(12),
while
other
studies
reported
higher
recurrence
rate
(7,
13).
Regarding
open
excision,
McEvedy
(1999)
reported
40
%
recurrence
rate
(14),
Jacobs
and
Govaers
(2006)
reported
28
%
and
Dias
et
al
(2007)
39
%
recurrence
rate
(3,
15).
We
had
a
recurrence
rate
of
24
%
in
our
study.
The
variability
in
results
to
some
extent
seems
to
be
surgeons
dependent.
Recurrence
rate
after
aspiration
and
injection
of
different
agents
are
higher
and
least
with
Silk
thread
passed
through
the
ganglion.
Gerhard
et
al
reported
85
%
recurrence
rate
after
hyaluronidase
injection
aspiration.
McEvedy
(1999)
reported
80
%
recurrence
rate
after
sclerosant
(14).
Derbyshire
(1966)
reported
60-85%
recurrence
rate
after
aspiration
and
injection
of
steroid
(16).
We
have
low
recurrence
of
43
%
after
aspiration
and
injection
of
methylprednisolone
compared
to
other
studies.
Arthroscopic
resection
of
ganglion
of
wrist
originally
described
by
Osterman
and
Raphael
(1995)
is
technically
difficult
and
demanding
(17).
Different
series
of
arthroscopic
resection
wrist
ganglion
have
shown
promising
results.
We
did
not
have
any
significant
complication.
Reviewing
the
literature
and
with
our
results
it
seems
Silk
thread
passed
through
the
ganglion
has
better
results
in
comparison
with
other
methods
of
treatment
and
is
an
acceptable
option
in
our
setup.
In
this
study
we
have
concluded
that
recurrence
rate,
postoperative
joint
stiffness
and
pain
resolution
was
least
in
a
new
method
technique
comparing
with
other
classical
surgical
and
non-surgical
groups.
Further
studies
with
more
patients
are
needed
to
elucidate
the
clinical
impact
of
Silk
thread
passed
in
cross
manner
in
the
management
of
wrist
ganglion.
1-
Burke
FD,
Melikyan
EY,
Bradley
MJ,
Dias
JJ.
Primary
care
referral
protocol
for
wrist
ganglia.
Postgraduate
Medical
Journal
2003;
79(932):
329-331.
2-Dias
J,
Buch
K.
Palmar
wrist
ganglion:
does
intervention
improve
outcome?
A
prospective
study
of
the
natural
history
and
patient-reported
treatment
outcomes.
Journal
of
Hand
Surgery
2003;
28(2):
172-176.
3-Dias
JJ,
Dhukaram
V,
Kumar
P.
The
natural
history
of
untreated
dorsal
wrist
ganglia
and
patient
reported
outcome
6
years
after
intervention.
Journal
of
Hand
Surgery
2007;
32E(5):
502-508.
4-Limpaphayom
N,
Wilairatana
V.
Randomized
controlled
trial
between
surgery
and
aspiration
combined
with
ethylprednisolone
acetate
injection
plus
wrist
immobilization
in
the
treatment
of
dorsal
carpal
ganglion.
Journal
of
the
Medical
Association
of
Thailand
2004;
87(12):
1513-1517.
5-Lowden
CM,
Attiah
M,
Garvin
G,
Macdermid
JC,
Osman
S,
Faber
KJ.
The
prevalence
of
wrist
ganglia
in
an
asymptomatic
population:
magnetic
resonance
evaluation.
The
Journal
of
Hand
Surgery
2005;
30(3):
302-306.
6-Tallia
AF,
Cardone
DA.
Diagnostic
and
therapeutic
injection
of
the
wrist
and
hand
region.
American
Family
Physician
2003;
67(4):
745-750.
7-Thommasen
HV,
Johnston
CS,
Thommasen
A.
Management
of
the
occasional
wrist
ganglion.
Canadian
Journal
of
Rural
Medicine
2006;
1(1):
51-52.
8-Gundes
H,
Cirpici
Y,
Saelak,
Muezzinoglu
S.
Prognosis
of
wrist
ganglion
operations.
Acta
Orthopaedica
Belgica
2000;
66(4):
363-367.
9-Mathoulin
C,
Hoyos
A,
Pelaez
J.
Arthroscopic
resection
of
wrist
ganglia.
Hand
Surgery
2004;
9(2):
159-164.
10-Povlsen
B,
Tavakkolizadeh
A.
Outcome
of
surgery
in
patients
with
painful
dorsal
wrist
ganglia.
Hand
Surgery
2004;
9(2):
171-173.
11-
Angelides
AC,
Wallace's
PF.The
dorsal
ganglion
of
the
wrist.its
pathogenesis
,gross
and
microscopic
anatomy
,and
surgical
treatment
.
JHand
Surgery
.2006;1;228235.
12-
Clay
NR,
Clement
DA,The
treatment
of
dorsal
wrist
ganglion
by
radical
excision;
JHand
Surg
2008;13;187-91.
13-Singhal
R,
Angmo
N,
Gupta
S,
Kumar
V,
Mehtani
A..
Ganglion
cysts
of
the
wrist:
A
prospective
study
of
a
simple
outpatient
management.
Acta
Orthopaedica
Belgica
2005;
71(5):
528-534.
14-
McEvedy
BV,The
simple
ganglion
:A
review
of
modes
of
treatment
and
an
explanation
of
the
frequent
failures
of
surgery;
LANCNT
1999;16;266;1356
15-
Jacob
LG,Govaers
KJ,
The
volar
wrist
ganglion
:Just
a
simple
cyst?
JHand
Surg
2006;11;21-6.
16-
Derbyshire
RC,
Observation
on
the
treatment
of
ganglion
,with
a
report
on
methylprednisolone
AM
J
SURG
1966
;112,635-6.
17-Osterman
AL,
Raphael
J.
Arthroscopic
resection
of
dorsal
ganglion
of
the
wrist.
Hand
Clin.
1995
Feb;11(1):7-12.
|
|
.................................................................................................................

|
| |
|
