|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
|
|
|
|
........................................................ |
Original
Contribution / Clinical Investigation
|
|
<-- Lebanon, Saudi Arabia, Algeria, UK,
Dubai, Qatar -->
The
dos and don’ts of painful diabetic peripheral
neuropathy: Primary care guidelines for the
Middle East and North Africa
[pdf
version]
Camille Aizarani , Ashraf A. Amir, Zoulikha
Benchouk, Muneer A. Abu Al-SamenMohamed Farghaly,
Adnan Kandil, Rayaz A. Malik
<-- Iran -->
Effect
of electro-acoustic factors on the continuous
use of hearing aid in hearing impaired children
under 15 years
[pdf
version]
Mansour Nazari Chafjiri, Nikta Hatamizadeh,
Asghar Makarem, Masoud Karimloo
<-- Iran -->
Comparative
study of the effects of narrative therapy and
play therapy by group approach on inhibiting
impulsivity, reducing aggression and increasing
interpersonal relations
[pdf
version]
Sepideh Kafili Kasmaei, Farhad Asghari
|
........................................................
International Health
Affairs
........................................................
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| June 2017 - Volume
15, Issue 4 |
|
|
Effect of electro-acoustic
factors on the continuous use of hearing aid
in hearing impaired children under 15 years
Mansour Nazari Chafjiri (1)
Nikta Hatamizadeh (2)
Asghar Makarem (3)
Masoud Karimloo (4)
(1) Welfare
Organization of Rasht, Rasht, Iran
(2) University of Welfare and Rehabilitation
Sciences, Tehran, Iran
(3) Welfare Organization of Tehran, Tehran,
Iran
(4) University of Welfare and Rehabilitation
Sciences, Tehran, Iran
Correspondence:
Mansour
Nazari
Chafjiri
Welfare
Organization of Rasht,
Rasht,
Iran
Email: mansour1347n@yahoo.com
|
Abstract
Objective: The
aim of this study was to evaluate the
effect of electro-acoustic factors (noise,
distortion, feedback) on the continuous
use of hearing aids in children under
15 years.
Method: This
study was conducted based on a causal
- comparative approach and by descriptive
- analytical techniques using a questionnaire.
In total,168 children under 15 years affected
by bilateral hearing loss, and who had
used a hearing aid for at least one year
and supported by welfare organization
of Rasht, were selected as the statistical
population. The data obtained was collected
using self-administered questionnaires
filled out by both children and parents
together.
For statistical analysis, both analytical
and descriptive techniques were used.
The obtained data were summarized as one,
two and three dimensional tables. For
data analysis the t- test and variance
analysis techniques were performed.
Results: The
obtained results showed that ear resonating
(buzz construction ), hearing aid whistling,
and annoying hearing of ambient sounds
had an inverse relationship with the average
hours of daily usage of hearing aid.
Decreasing ability of understanding speech
in the presence of noise is one of the
main complaints in hearing impaired people.
Effective communication in complex listening
environments requires the health of peripheral,
central and cognitive auditory system.
If the process fails at any point in these
devices the ability of understanding speech
reduces.
Speech is a very complex audio-signal
consisting of sections and acoustical
properties. Each of the sections have
great importance for the formation of
correct speech understanding. An impairment
in organizing input hearing understanding,
similar to the incidence of hearing loss,
can cause significant implications in
the understanding and identification of
complex auditory signals, such as speech
and music. Separating these different
sounds when simultaneously presented is
normally carried out on the basis of their
different frequencies and the harmonic
relations of each of them.
It seems that small adjustments for the
hearing aid and the solving of electro-acoustic
problems can improve its daily usage(4).
Key words:
Electro-acoustic factors, hearing impaired,
hearing aid, continuous usage of hearing
aid
|
Hearing is one of most important of human senses,
and provides much information for humans, so any
hearing impairment could affect the personal aspects
of human life. Natural and good hearing is crucial
for appropriate speech also (3).
Measurement and analysis of acoustic parameters
is one of the objective assays (1). Each receptive
human needs to recognize the source of sound production,
especially speech, in order to integrate information
of their surrounding environment which includes
the complexity of various sounds. For this purpose,
acoustical properties of sound sources should
be separate and classified correctly (13). Hearing
impairment leads to delay in development of hearing
and speech communicational skills, and under special
situations leads to inhibition of development
of personal-social aspects of life. Then it leads
to problems such as emotional, job, educational,
mental, and social problems. Two effective factors
seem to be the hearing loss amount and the age
at incidence of hearing loss (3). Studies have
shown that children with bilateral profound hearing
loss cannot improve their oral capabilities because
of the failure to appreciate their surrounding
sound environment. Therefore, collection of the
maximum remaining hearing for these children is
important (10).
Hearing loss is one of affective causes on impairing
speaking skills. Acoustic stimulation can positively
affect the child's nervous development by allowing
them to hear speech signals effectively because
in deaf children who cannot hear speech and live
in a silent environment, viable synapses for hearing-oral
skills will drop and gradually be lost (14).
Development of language, speech, education, training
skills, social skills and job skills depend on
hearing sense in the early years of life. The
first step for rehabilitation of the deaf and
hearing impaired person is equipment to assist
their hearing (11).
A hearing aid is the most frequently employed
item of equipment for improvement of hearing loss
and is the key to improve the input voices. Hearing
aids cannot guarantee the hearing of all voices
and sounds. The type, its operation and ear suitability
are the critical factors on its efficiency (5).
Usage of a hearing aid by patients is more important
than prescribing of a hearing aid for them. When
the patient does not always use a hearing aid,
we should answer some important questions about
the extent and causes of patient's satisfaction/dissatisfaction
with their hearing aid. Identifying these should
be followed by finding the appropriate way to
overcome the non-use of hearing aids.
Based on unofficial studies and observation, it
is found most Iranian deaf students do not use
a hearing aid. Hence their educative-communicational
disabilities are at least partly due to non-use
of hearing aid. They give many excuses for this.
For example, they say I forgot the hearing aid,
it is broken, I lost it, the battery has run down
etc. However in most cases, the hearing aid is
in their bag, but they are not interested in using
it (2).
Katz (1994) revealed 25-50% of hearing aids are
not used at the desired level in American children.
Katz (1994) studied the hearing aids situation
in different American schools for 15 years and
showed that most causes for failure of routine
use of hearing aid are impaired batteries, non-fit
frame, broken control keys, high harmonic distortion
and non-friendly repair systems (9).
Kochkins (1994) showed 18% of hearing impaired
and deaf persons do not use their hearing aid(9).
Karstizer (1973) studied the ways of successful
application of hearing aids and showed that most
patients are satisfied only when they are talking
with one person. They have some problems when
they talk with two or more persons. Meanwhile,
they are satisfied when they are at home alone,
during shopping and general meeting, however this
satisfaction decreases significantly during trips
and work (6).
Kiese-Himmel et al (2000) evaluated the hearing
aid acceptance among children. They revealed children
with unilateral profound hearing loss, use hearing
aids less than children with bilateral profound
hearing loss (8).Non-appropriate adjustment of
hearing aid and non-maximal output are the most
causes of its non-acceptance.
Franks and Beckman (1982) showed one of the causes
of 88% of elderly patients for rejection of their
hearing aid is high amplification of voices. Although
these authors believed non-appropriate adjustment
of hearing aid output had not led to its non-acceptance,
it has a negative experience for patients (4).
Schuchman and Montgomery (1978) studied some questions
about new users of hearing aids. They included
430 patients in their study and concluded 63%
of causes of non-compliance is noise feedback
(12). Since there is a difference between other
studies and our Iranian people from the viewpoint
of age, culture and society conditions, we investigated
the effect of electro-acoustic factors on the
continuous use of hearing aid in hearing impaired
children under 15 years.
This trial was a causal-comparative study.
A total of 168 hearing impaired children under
15 years who were affected by bilateral hearing
loss, supported by welfare organization of Rasht,
Iran and who used hearing aid for at least one
year, were selected as the statistical population.
All patients are new users of hearing aids (2011-2014).
Obtained data were collected using self-administered
questionnaires, filled out by both children
and parents together.
For assessment of stability and robustness of
questionnaires, 10% of the sample population
filled them out again after one month. The questionnaires
had more than 80% compatibility. For assessment
of validity of questionnaires, the content was
assessed by hearing aid experts and a specialist
and then edited to remove objections.
A list was prepared using all new (2011-2014)
users of hearing aids who received their hearing
aid from welfare organization of Rasht, Iran.
The patients were sorted based on hearing aid
type. There were 196 patients, although we could
get access to addresses and telephones for only
168 patients. All 168 patients were therefore
chosen as the sample. We could access home telephone
for 57 patients. We contacted them and requested
a visiting appointment at the welfare organization
of Rasht, Iran. Thereafter 38 patients came
into the welfare organization of Rasht, Iran
and filled out the questionnaire. Also 63 patients
come into the welfare organization of Rasht,
Iran for routine checks of frame, battery etc
and filled out the questionnaire. Some questionnaires
were sent by regular post to the home addresses
of patients and thus we collected 53 filled
questionnaires by post also. Finally, we visited
the home address for 14 patients and filled
out the questionnaire at their home (38+63+53+14=168).
If both hearing impaired and parents were illiterate,
we filled out the questionnaire by means of
interview.
For statistical analysis, both analytical and
descriptive techniques were used (absolute and
relative frequency, average, and middle). Obtained
data were summarized as one, two and three dimensional
tables. For data analysis the t- test and variance
analysis techniques were performed. SPSS software
was used for statistical analysis.
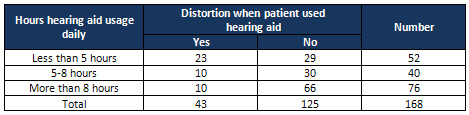
Based
on
Table
1,
it
is
shown
that
the
individuals
with
less
than
5
hours
hearing
aid
usage
daily
had
the
most
distortion;
the
individuals
with
more
than
8
hours
hearing
aid
usage
daily
had
the
lowest
distortion.
Table
1:
Frequency
of
distortion
when
patient
used
hearing
aid
based
on
hours
of
hearing
aid
usage
daily
Table
2:
Average
of
daily
hearing
aid
usage
based
on
distortion

From
Table
2
it
is
shown
that
average
of
daily
hearing
aid
usage
for
patients
who
had
distortion
is
5.8
hours
and
average
of
daily
hearing
aid
usage
for
patients
who
had
no
distortion
is
8.
So
the
differences
of
these
two
values
is
significant
(t=3.797;
P-value=0.000).
Therefore
the
null
hypothesis
(average
of
daily
hearing
aid
usage
for
patients
who
had
and
had
not
distortion
is
equal)
is
rejected.
It
is
concluded
that
distortion
affects
the
average
daily
hearing
aid
usage.
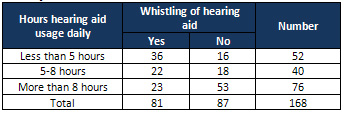
From
Table
3
it
is
shown
that
among
the
total
of
168
studied
patients,
that
81
individuals
(48.2%)
experienced
whistling
of
the
hearing
aid;
and
most
of
whom
used
the
equipment
for
less
than
5
hours
daily,
whereas
23
(28.4%)
patients
used
it
more
than
8
hours
daily.
On
the
other
hand,
between
87
patients
who
did
not
have
whistling
of
hearing
aid,
53
(60.9%)
individuals
used
it
more
than
8
hours
daily.
Table
3:
Frequency
of
whistling
of
hearing
aid
based
on
hours
of
hearing
aid
usage
daily
Table
4:
Hours
of
hearing
aid
usage
daily
based
on
whistling
of
hearing
aid

Table
4
shows
hours
of
hearing
aid
usage
daily
for
patients
who
were
faced
with
whistling
of
their
hearing
aid
is
6.0
hours,
and
for
patients
who
did
not
face
whistling
it
is
8.6
hours.
So
the
differences
of
these
two
values
is
significant
(t=-4.741;
P-value=0.000).
Therefore
the
null
hypothesis
(average
of
daily
hearing
aid
usage
for
patients
who
had
and
had
not
whistling
of
hearing
aid
is
equal)
is
rejected.
It
is
concluded
whistling
of
hearing
aid
definitely
affects
the
average
of
daily
hearing
aid
usage.
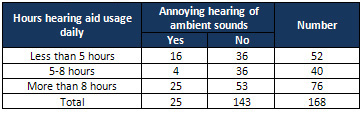
From
Table
5
it
is
shown
that
among
the
total
of
168
studied
patients,
25
individuals
(14.9%)
had
noise,
of
whom16
individuals
were
those
who
used
their
aid
less
than
5
hours
daily.
Table
5:
Frequency
of
annoying
hearing
of
ambient
sounds
based
on
hours
hearing
aid
usage
daily
Table
6:
Hours
hearing
aid
usage
daily
based
on
annoying
hearing
of
ambient
sounds
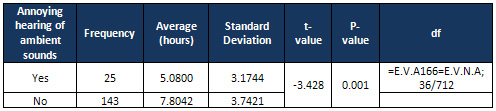
From
Table
6
it
is
shown
that
hours
of
hearing
aid
usage
daily
for
patients
who
experienced
annoying
ambient
sounds
was
5.0
hours,
whereas
patients
who
did
not
face
annoying
ambient
sounds
was
8.6
hours.
So
the
differences
of
these
two
values
is
significant
(t=-3.428;
P-value=0.001).
Therefore
the
null
hypothesis
(average
of
daily
hearing
aid
usage
for
patients
who
had
and
had
not
annoying
hearing
of
ambient
sounds
is
equal)
is
rejected.
It
is
clear
that
annoying
hearing
of
ambient
sounds
does
affect
the
average
daily
hearing
aid
usage.
The
aim
of
the
present
study
was
the
investigation
of
the
effect
of
electro-acoustic
factors
on
the
continuous
use
of
hearing
aid
in
hearing
impaired
children
under
15
years
supported
by
welfare
organization
of
Rasht
city.
In
one
study
about
problems
during
hearing
aid
usage
Raanaei
and
Goorabi
(1994)
revealed
that
among
932
impaired
veterans,
874
(93.7%)
individuals
did
not
have
a
hearing
aid
or
did
not
have
a
problem
in
hearing
aid
usage.
Meanwhile
0.85%
individuals
had
nonsense
sounds
in
their
hearing
aid
(12).
In
the
present
study,
13.7%
individuals
faced
rustle
and
nonsense
sounds.
Raanaei
and
Goorabi
(1994)
showed
0.43%
individuals
noted
high
and
annoying
sounds
(12),
whereas
in
our
study
14.9%
individuals
faced
high
and
annoying
sounds.
Raanaei
and
Ghoorabi
(1994)
showed
0.75%
individuals
reported
whistling
of
their
hearing
aid
(12),
whereas
in
our
study
48.2%
individuals
faced
this.
Akbarlou-Shabgahi
(2001)
studied
513
Tehran
deaf
students
and
revealed
16.98%
students
did
not
use
their
hearing
aid,
since
they
rejected
uncomfortable
sounds
from
it,
and
also
11.32%
students
rejected
hearing
aid
use
because
of
nonsense
and
non-clear
sounds.
In
our
study
13.7%
individuals
had
nonsense
and
non-clear
sounds,
14.9%
individuals
were
faced
with
uncomfortable
sounds
from
the
hearing
aid
and
25.6%
individuals
were
faced
with
distortion
of
hearing
aid.
Therefore
there
are
fundamental
differences
between
our
and
their
study.
It
could
be
due
to
statistical
population
and
sample
size.
The
results
showed
that
the
ear
resonating
(buzz),
whistling
of
hearing
aid,
and
annoying
hearing
of
ambient
sounds
had
an
inverse
relationship
with
the
average
hours
of
daily
usage
of
hearing
aid.
One
of
the
important
factors
on
continuous
usage
of
hearing
aid
is
whistling
of
hearing
aid.
This
problem
is
due
to
the
hearing
aid's
frame
mostly.
In
powerful
hearing
aids
care
should
be
taken
that
the
frame
can
snugly
fit
with
the
ear
canal.
Most
available
hard
frames
are
not
appropriate.
Hence
the
costs
should
cover
the
provision
of
soft
frames
in
welfare
organizations.
Meanwhile,
for
growing
children,
new
frames
should
be
prepared
regularly
due
to
gradual
development
of
ear
canal.
Other
factors
relevant
to
hearing
aid
whistle
problems
are
disturbance
of
the
frame's
tube,
speaker's
tube,
microphone,
ear
wax
etc
and
the
non-appropriate
adjustment
of
the
hearing
aid,
etc.
These
factors
could
be
overcome
by
using
appropriate
consultation
and
education,
periodical
review
of
hearing
aid,
and
periodical
inspection
of
ear
canal.
In
addition,
electro-acoustic
factors
contribute
to
the
annoying
hearing
of
ambient
sounds.
This
factor
could
be
detected
by
audiological
tests
(SRT-MSL-SDS-USL)
and
the
study
of
the
dynamic
range
by
audiologists
so
that
the
problem
could
be
overcome
by
the
prescription
of
an
appropriate
hearing
aid.
Based
on
our
findings,
it
is
recommended
that
welfare
organizations
should
provide
hearing
aids
that
have
minimum
internal
noise
and
also
recommend
the
provision
of
digital
hearing
aids
that
are
adjustable,
based
on
the
type
and
extent
of
hearing
loss.
It
is
recommend
that
analogue
and
Digitrim
hearing
aids
should
be
replaced
by
automatic
and
multi-program
hearing
aids.
Providers
should
pay
attention
to
shape,
size,
quality
and
patient's
requirements.
Meanwhile
it
is
necessary
to
educate
on
careful
use
and
daily
control
of
the
hearing
aid
by
audiologist
experts.
It
is
recommended
that
there
is
periodical
inspection
of
patients
(ear
canal
control
for
ear
wax
etc)
such
as
planned
and
monthly
hearing
aid
control
by
audiologist
experts.
We
recommend
the
preparation
of
a
special
form
to
order
a
hearing
aid
evaluation,
to
collect
patients'
ideas
and
also
monitor
the
hearing
aids
each
six
months.
1.
Akbari,
E.,
Ghorbani,
A.
et
al.,
2014.
Differences
of
acoustic
properties
of
functional
disorder
of
voices.
Journal
of
Paramedical
and
Rehabilitation
of
Mashhad.Volume
3.Issue
2.
2.
Akbari-Shabgahim
N.
2001.
Study
of
availability
and
use
of
hearing
aid
in
deaf
school
(Tehran
city).Exceptional
children
Research
Center
Press.
Tehran.
Iran.
3.
Dillon,
H.
2002.
Hearing
Aids.(2,478):-595p.
4.
Franks.
JR,
Beckmann.
NJ.
1982.
Rejection
of
hearing
aids:
Attitudes
of
a
geriatric
sample,
Ear
hear.
5.
Ghojaghi,
A.
1991.
What
you
know
about
your
ear?
Jihade
Daneshgahi
Press
of
Medical
University
of
Shahid
Beheshti.
Tehran,
Iran.
6.
Jafari,
Z.,
Abasalipour-Kabireh,
P.
2001.
Investigation
on
prescription
and
fitting
of
hearing
aids.
Nashrva
Tabligh
Bashari
Press,
Tehran,
Iran.
7.
Katz,
J.
1994.
Hand
book
of
clinical
audiology.(839p)
8.
Kiese-Himmel
C,
Ohlweins,
Kruse
E,
2000.Acceptance
of
wearing
hearing
aids
by
children,HNO,48(10):758-64
9.
Madell,
JR.
1998.Behavioral
Evaluation
of
hearing
in
infants
and
young
children,
New
York.
10.
Mirza-aghabeig,
S.,
Molali,
G.,
Taheri,
M.,
Jafari,
S.
2015.
Study
of
effectiveness
of
cued
speech
on
oral
skill
of
subject
memorize,
major
information
and
successive
of
story
in
hearing
impaired
students
treated
late
cochlear
implant.
Journal
of
Welfare
and
Rehabilitation
Sciences.
Volume
16.
Issue
1.
11.
Northern,
J.,
Downs,
MP.2002.
Hearing
in
children.
406p
12.
Raanaei,
M.
Goorabi,
K.
1999.
Descriptive
study
of
audiogram
sheets
and
prescription
of
hearing
aid
in
veteran.
Iranian
Audiology
Journal.
Volume
11
and
12.
13.
Talebi,
H.,
Mousavi,
A.,
Lotfi,
Y.,
Faghihzadeh,
S.,
2014.Problems
of
simultaneous
separation
of
speech
voices.
Research
journal
of
Rehabilitation.
Volume
15,
Issue
1.
14.
Valizadeh,
A.,
Gouhari,
N.,
Fatehi,
N.,
Yavari,
A.
2015.
Comparison
of
some
speech
properties
of
hearing
impaired
high
school
students.
Journal
of
Paramedical
and
Rehabilitation
of
Mashhad.
Volume
4.Issue
4.
|
|
.................................................................................................................

|
| |
|
