|
Comparative study of
the effects of narrative therapy and play therapy
by group approach on inhibiting impulsivity,
reducing aggression and increasing interpersonal
relations
Sepideh Kafili Kasmaei (1)
Farhad Asghari (2)
(1) Department
of Counseling, North Tehran Branch, Islamic
Azad University, Tehran, Iran
(2) Department of Counseling, University of
Guilan, Rasht, Iran.
Correspondence:
Farhad
Asghari
Department of Counseling,
University of Guilan,
Rasht,
Iran
Email: farhad.asghari@gmail.com
|
Abstract
The main objective of this study was to
compare the efficacy of group narrative
therapy and play therapy on inhibiting
impulsivity, reducing aggression and increasing
interpersonal relations. The research
methodology was a quasi-experimental approach.
The study population consisted of primary
school parentless boys in Welfare Centers
in the city of Rasht. The sample in this
study included 30 primary school parentless
male children (7-11 years old) who had
been diagnosed with aggressive behaviors
disorders, lack of interpersonal relationships
and inability to control impulses, by
the consultants of welfare centers in
Rasht. Using the available sampling method,
the sampled members were randomly divided
into three 10-subject groups of experimental
narrative therapy group, experimental
play therapy group and the control group.
The research tools included overt and
relational aggression questionnaire for
primary school children, Hershfield impulsivity
scale and children self-efficacy scale
in interpersonal relationships with peers.
The results showed that both treatment
methods, namely group narrative therapy
and play therapy are effective in inhibiting
impulsivity, reducing aggression and increasing
interpersonal relations at the level of
(P < 0.01). Separately compared based
on the results, we can conclude that the
play therapy method is a more effective
approach regarding the variables of impulsivity
and aggression in comparison with the
narrative therapy, while these two treatment
methods are not statistically significant
on variable of interpersonal relations.
The group play therapy method can be used
to reduce aggression and impulsive behaviors.
Keywords: Narrative
therapy, Play therapy, Impulsivity, Aggression,
Interpersonal relations
|
Attention to children's growth and development
is important in terms of different aspects. Children,
as future-makers of their own society, will be
useful to the society when they have grown and
been fostered in a healthy, growing and safe family
environment. But in the meantime, some children
are deprived of the blessings of developing in
the family environment and their growth is faced
with challenging conditions. One of the problems
of social life is addressing the issues of children
that have been orphaned for some reason. Most
orphaned children have lost their parents or one
of them as a result of various events and accidents,
or for reasons such as the parents do not have
the competence necessary to foster their own children
and the children have no in-laws or relatives
able to take custody of them. After breaking up
of families because of divorce or death of a parent,
it has frequently been seen that innocent children
have been entrusted to institutions for parentless
children and children with irresponsible caretakers
in the name of poverty or inability of one of
the parents, or their remarriage and have deprived
them of the luxury of having families [1].
Living in orphanages creates many challenges in
the process of child development that could adversely
affect various aspects of children's psychological
development [2]. Due to deprivation of a natural
family environment, the parentless children and
children with irresponsible caretakers living
in the orphanages' nursery encounter a variety
of damage and deprivation. Thus, as children constitute
a major and important group of our country's population,
accurate and complete recognition of this class
would be effective in helping to create material
and spiritual grounds for their emotional and
psychological growth and development [3].
Children living in welfare centers have a wide
range of behavioral and emotional problems, including
a higher prevalence of aggression [4]. Therefore,
paying special attention to this group of children
and treatment of aggressive behaviors in this
particular environment seems to be much more important.
Defining the term aggression is very difficult.
Since, neither the aggressor's intention and purpose
nor the feelings and perceptions of the victim
can be observed directly. The aggressive behavior
is profoundly influenced by the social judgments
of the aggressor and the victim of aggression.
Aggression usually refers to a behavior with the
intention of harming others or destroying the
property of individuals [5]. Aggression can be
physical, such as kicking, pushing or biting,
or it can be verbal, such as backbiting, humiliation,
insulting and slander [6]. In other words, aggression
arises from the objective to harm and is a tendency
to participate in the traumatic physical and psychological
actions to control the actions of others [7].
The other problem of these children is impulsivity.
Impulsivity has been described as intense tendency
to repeat a behavior, without sufficient thinking
against internal and external stimuli [8].
Impulsivity has been mentioned in some texts as
risky behaviors [9]. Impulsivity in these children
is such that these children respond to all questions
before they finish. Waiting for their turn is
very difficult for them. They often intrude on
the work of others, and may jump in the middle
of others' talk or play. These children are very
restless and impatient due to high impulsivity,
and these features cause disturbance in their
social and academic situations [10]. In other
words, impulsivity is a behavior without thinking
and realizing and acting by instinct, regardless
of the consequences of a behavior, and includes
a wide range of behaviors that occur with a high
amount of risk and without spending the time for
planning or considering various aspects and possible
consequences of that behavior, which often leads
to adverse consequences [11].
These children lack intimate relationships with
their friends due to being aggressive and impulsive.
For the same reason, they grapple with many problems
in their interpersonal relationships [12]. Interpersonal
communication is a process through which, we share
information, ideas and emotions via verbal and
nonverbal messages with others. These communications
are often face to face communications with a limited
number of participants (usually two) [13]. Due
to not respecting turns and game rules, failure
to follow instructions, disturbing the order and
impulsive behaviors, these children are rejected
by their friends, and negative consequences that
they frequently get from their environment would
damage their self-confidence and predispose them
to depression and anxiety. Hence, one of the signs
of mental health is the presence of healthy interpersonal
relationships. In this case, the children's social
contact goes beyond the family and involves the
communication with their peers' world. Connecting
with peers is of great importance even for little
children since communication with peers, especially
friends, plays an important role in their life
and evolution. Friends are the most important
source of companionship and camaraderie[14].
One method of treatment for such children can
be play therapy. Children should be seen and recognized
based on a developmental approach. They are not
small adults. Their world is one of objective
realities, and their experiences are often expressed
through playing. Therapists, who seek to facilitate
the translation of children's emotional world
when exploring such, need to leave their real
and verbal world and step down into the cognitive-affective
world of children. The usual way of communication
for children is playing and activities [15]. In
this type of treatment, the effective therapeutic
relationship with children is well established
through playing and games. Playing is a way through
which conflicts can be solved and feelings can
be expressed. Toys realize this process; for they
are indeed ways that the children express themselves.
The children's free games somehow express what
they want to do. When children play freely and
without guidance, they show a period of independent
thought and action. They release feelings and
attitudes that pressure themselves to get free
[16]. Feelings and ideas that may be very threatening
for children when directly expressed can be safely
projected through toys that children pick up by
themselves. Instead of verbal expression of thoughts
and feelings, the child can bury a doll in the
sand, shoot it, or hit it, which may be representing
his or her younger brother [17].
In addition to the play therapy, in recent year,
storytelling approach is widespread for understanding
human behavior in different fields of psychology.
Because of certain circumstances of childhood
in terms of their cognitive abilities, the children
can further use narrative therapy method. In fact,
closeness and proximity of children to major interpersonal
events in everyday life and their immersion in
sensory and objective aspects of experiences have
given a stronger influence to these events in
their stories of lives [18]. Narrative therapy,
as a treatment technique, has wide dimensions
and is not limited only to treating the psychological
problems of children. In narrative therapy, it
is assumed that the change in the language and
literature of life stories would lead to alterations
in the individual's life meaning, and create new
opportunities for treating and relationships with
others through changing the life stories [19].
Generally, children identify with the characters
in the story, and with making hypotheses and providing
different solutions to resolve the challenges
of the story characters, they grow their problem
solving skills [20]. By understanding the relationship
between the story subject and their life theme,
children can directly think about their issues
and find solutions for them [21]. The relationship
between the storyteller and the listener is an
important part of the narrative therapy, which
provides the children with an opportunity to tell
their story both emotionally and cognitively.
Narrative therapy, in addition to strengthening
the parents - children relationship, shapes a
more integrated self in the children [22].
Therefore, considering the importance of the educational
aspect of story and storytelling as well as the
play therapy as an art of communicating with children,
this study aimed to assess and compare the effectiveness
of narrative therapy and play therapy through
a group approach on inhibiting impulsivity, reducing
aggression and increasing interpersonal relationships
by using the principles of playing as a valuable
and effective means.
Population, sample, sampling method
This was a quasi-experimental study with a pre-test
and post-test design by a control group. The
independent variable was group narrative therapy
and play therapy, each applied separately and
distinctly only in the experimental group and
their effects on inhibiting impulsivity, reducing
aggressive behaviors and improving interpersonal
relationships of parentless primary school boy
children in the experimental group, were compared
with the control group. The study population
consisted of primary school parentless boys
in Welfare Centers in the city of Rasht, in
the academic year of 2016-2017. The sample in
this study included 30 primary school parentless
male children (7-11 years old) who had been
diagnosed with aggressive behaviors disorders,
lack of interpersonal relationships and inability
to control impulses, by the consultants of welfare
centers in Rasht, who had clinical and medical
records in private clinics based on the same
diagnosis. In addition, by doing semi-structured
interviews with children, caregivers and educators
of children in the care centers, based on the
fifth edition of the Diagnostic and Statistical
guidance on the criteria of Mental disorders
(DSM-5), the presence of these disorders were
confirmed in the children. The samples were
selected by convenience sampling method from
the welfare centers in Rasht. Then they were
randomly divided into two experimental and control
groups, and were asked to answer overt and relational
aggression questionnaire for primary school
children, Hershfield impulsivity scale and children
self-efficacy scale in interpersonal relationships
with peers. Subsequently, the samples were randomly
divided into three 10-subject groups of experimental
narrative therapy group, experimental play therapy
group and the control group. Then the children
in the experimental group separately participated
in ten, one and a half hour sessions, of narrative
therapy and play therapy. After the intervention
sessions, the children were asked again to answer
the same previous questionnaires.
Research Tools
Overt and relational aggression questionnaire
for primary school children
This questionnaire contains 21 statements on
relational and overt aggression that is completed
by teachers and educators. The statements are
set as such to cover varying degrees of severity
of aggression and are rated based on the occurrence
rate of behavior. French and Janson (2002) define
aggression consisting of three dimensions of
manipulating interpersonal relations, spreading
malicious rumors and rejection of others. To
prepare the relational aggression questionnaire,
each of the above dimensions has been adapted
to Iranian culture, and the questionnaire statements
have been classified in these three dimensions.
Respectively, 2, 4 and 2 statements have been
considered for manipulating relationships, peer
rejection and gossiping [23].
In the dimension of overt aggression, some statements
are designed regarding physical aggression (7
statements), verbal reaction (3 statements)
and proactive aggression (3 statements). Scoring
is done on a Likert scale from 1 to 4. Then
the scores of each statement in each factor
are summed and the factor scores were obtained
and compared with the mean and standard deviation
of scores of girls and boys. The scores higher
than one standard deviation above the normal
range in each factor were seen as aggression.
The Cronbach's alpha coefficient for the whole
questionnaire in this study is equal to 0.91
and is highly desirable. The Cronbach's alpha
coefficient for physical, relational and reactive
aggression is equal to 0.86, 0.83 and 0.81,
respectively [24]. According to the overt and
relational aggression questionnaire for primary
school children, in physical aggression, the
scores higher than 8 for girls and the scores
higher than 10 for boys were considered aggressive.
In relational aggression, the scores higher
than 18 for girls and the scores higher than
17 for boys were considered aggressive. In verbal
- proactive reactive aggression, the scores
higher than 15 for girls and the scores higher
than 16 for boys were considered aggressive.
The reliability calculated in this study for
physical, relational and reactive aggression
was 0.81, 0.87 and 0.79, respectively.
Hershfield impulsivity scale
The impulsivity scale in 1965 by Hershfield
for evaluation of impulsivity in primary school
children was used. The tool has 19 items that
are set for its implementation in the form of
'properly - improperly'. In this tool, impulsivity
is defined as a desire to fidget, lawlessness
and indulging in violent games. The tool is
potentially made for children with control and
coping problems and externalizing disorders.
The reliability of this test, made by Hershfield
by test-retest method, is equal to 85%. Also,
in Saati's research (2016), the Cronbach's alpha
coefficient was obtained as 84% for the scale
[25]. The reliability calculated in this study
based on the Cronbach's alpha coefficient was
0.76.
Children self-efficacy scale in interpersonal
relationships with peers
The children self-efficacy scale in interpersonal
relationships with peers was developed by Wheeler
V. Ladd (1982) with the aim of measuring self-efficacy
of children in interpersonal relationships.
Any item of this scale is written as an unfinished
sentence where children must choose one of the
four options (Very Easy, Easy, Hard and Very
Hard) about the provided sentence due to their
status. The options are reversely scored, and
the score of each participant occurs in a range
from 22 (attainable minimum score) to 88 (attainable
maximum score).
The standardization of this test in Iran was
done by Hossienchari (2008), which results revealed
the realization of psychometric properties of
the scale used to assess self-efficacy in students.
The reliability coefficients of the total scale,
conflict subscale and no-conflict subscale were
0.87, 0.83 and 0.78, respectively [26]. The
reliability calculated in this study was 0.89
based on the Cronbach's alpha coefficient.
Procedure
In accordance with the planned educational program,
educational interventions were designed and
implemented. The experimental group was trained
in ten 90-minute sessions during seven weeks,
while the control group received no intervention.
The summaries of play therapy training sessions
are as follows:
First session
Before starting the group sessions, the children
were individually led into the play therapy
room in a session, which goals included reducing
their sensitivity to the play therapy room,
familiarity with it and familiarity and establishing
a good relationship with the therapist.
Second session
The group members were introduced to each other.
In this session, the children's adaptation with
the environment and each other was considered.
To establish friendship and safety, any game
suggested by children was played. In this particular
session, the therapist had the role of mediator
to have better communication between children.
Third session
Firstly, to prepare children to participate
in group games, mini basketball game and group
golf play were used. The aim of playing these
games was to create vitality and encouragement
of children for later games. Also, these games
were raised and selected for strengthening communication
skills, anxiety reduction and public participation.
Fourth session
In this session, wild and domestic animal toys
were used with the main purpose of encouraging
the children to talk and explore the quality
of their relationships with others and vice
versa. Other objectives were as follows: Discovering
the children's concerns about their relationships
in the future, discovering the main sources
of their depression and anxiety, the discovery
of fear or withdrawal from relationships with
others, and finally, discovering the factors
that have distanced them from the path of normal
development.
Fifth session
This session involved the review of playing
with toy animals in the previous session and
playing the performances that children were
willing to do in the last session, to bring
into this session. The purpose of doing the
play chosen by children was to investigate the
roots of children's problems, since the children
chose plays consistent with their current psychological
conditions.
Sixth Session
This session included the participation of children
and consultation with them about dramatic plays
of other children. The idea was to get children
familiar with different stories and learn the
ways to solve them so that in case of occurrence
of another problem, they will experience lower
levels of anxiety and depression.
Seventh session
It included playing with dough which is a valuable
tool in playing with children. When playing
with dough, children make important figures
in their lives in their own present, past and
future and interact with the characters, express
feelings and re-experience.
Eighth session
It included the imaginary trip game. The most
important aspect of these imaginary journeys
is to encourage the children to tell their stories,
take a look inside themselves and others' behaviors
and find out the possible causes of some past
events. In this game, the fears of children
are identified, and based on their imagination,
the children travel to the present, past and
future and communicate with different characters
of their lives.
Ninth session
In addition to review, the imaginary trip play
helps them provide solutions for problems encountered
in the course of an imaginary trip and also
hear other children's comments, while they do
not think about the worthlessness of their opinions.
Tenth session
It consisted of review and revision of previous
sessions and was the end of the educational
intervention.
Overall routine of therapy sessions
Narrative therapy involved giving lectures on
the raised topics associated with the table
below and providing examples as well as practical
performing of techniques and interviews with
the group members.
Exclusive content of narrative therapy sessions
| Session |
Content |
| 1 |
Welcoming,
introducing the sessions' structure and
basic rules, introducing participants to
each other.
Storytelling of "Blatherer (Secret
telling) Heart" story: Accumulation
and lack of understanding and processing
of information and suffering from mental
disorders in humans.
Assignment: Find a story in which
a person with mental illness acts abnormally. |
| 2 |
Presenting
the selected story: "Develop how you
want it to grow."
Story building and working on metaphors:
Introduction: The therapist tells the children
that we want to go on a voyage and write
a story about the events of the trip. Choose
a title for this story.
Name three items that you want to take with
yourself on the trip.
Write a paragraph about farewell and those
present at the ceremony.
Put three confidential advices inside an
envelope and give it to a trusted person.
Assignment: If you replace the old
storyteller, how would you tell the story
and with what animal character? Write your
story. |
| 3 |
Presenting
the selected story: "The Pursuit of
Happiness"
Story building and working on metaphors:
Chapter One: What may we encounter on this
trip? Who will we face? What will be the
new climate conditions? Write a paragraph
about each.
Assignment: Write a story according
to the meaning and form of "The Pursuit
of Happiness" story. |
| 4 |
Presenting
the selected story: "Flight to New
Horizons"
Story building and working on metaphors:
Chapter Two: The ship is moving, and something
is in the water. Passengers are busy watching
the sea and surroundings on the deck. Suddenly,
someone screams that something is seen under
water. The participants must write a paragraph
about what they see underwater.
Assignment: Write about an experience
of your past life in the form of the story
"Flight to New Horizons". |
| 5 |
Presenting
the selected story: "Good but Not Perfect"
Story building and working on metaphors:
Chapter Three: A mysterious box is found.
The children will be asked to talk about
the nature of the box and its contents,
its owner, how to open its locks and whether
we should open it or not, and make notes
of their content in their notebook.
Assignment: Rewrite an experience
of your life in the form of the story "Good
but Not Perfect". |
| 6 |
Presenting
the selected story: "Changing behavioral
patterns"
Story building and working on metaphors:
Chapter Four: "Need for change"
It is night and the ship is moving. It is
reported to the captain that another ship
is crossing their path, and it does not
respond to any signals. They should act
as soon as possible, otherwise the ships
will collide. The children need to write
a paragraph about taking appropriate measures
to prevent the danger. They will write it
after a group discussion.
Assignment: Rewrite the selected
story about another animal other than crow.
Try to make friendship with animals like
cats, pigeons, etc. that run away from you,
and report the results. |
| 7 |
Presenting
the selected story: "Making friends
and keeping the friendship"
Story building and working on metaphors:
Chapter Six: A dream: Sea is calm and the
ship is moving and the passengers are asleep.
One of them is dreaming. Guess the dream
and write a paragraph about it.
Assignment: Write a paragraph about
the initial contact with your closest friend.
Make an interview with him/her and write
his/her opinions about yourself. |
| 8 |
Presenting
the selected story: "Do not drop the
handle"
Story building and working on metaphors:
Chapter Seven: Reaching a mysterious island:
The passengers are notified that because
of the past events, much time has been lost
and food and fresh water to continue the
journey are over. They are forced to get
off on the mysterious island near them.
The children should write a paragraph about
this mysterious island.
Assignment: Find an ant and follow
it until its nest. Summarize the statements
that the ant repeats by itself when working
in a paragraph |
| 9 |
Presenting
the selected story: "Let Joe do it"
Story building and working on metaphors:
Last chapter: Reaching the destination:
Finally, the ship arrives to its destination
and docks at the pier. The travelers had
a lot of work to do. Everyone gets busy
to quickly prepare themselves for returning
home. The children should write a paragraph
about their feelings and actions.
Assignment: Write a paragraph about
a skill that you think you can do better
than others.
How were you at the beginning? And, how
have you gained such a skill? Write another
paragraph. |
| 10 |
Review
of the program: Helping participants to
review and rewrite their story
Follow-up and evaluation of the treatment:
Obtaining feedback from participants about
the program and evaluation |
To
test
the
main
hypothesis,
the
analysis
of
covariance
(MANCOVA)
by
K
Matrix
method
was
used.
This
test
is
a
statistical
method
that
allows
you
to
examine
the
effect
of
the
independent
variable
on
the
dependent
variable,
while
eliminating
or
removing
the
effect
of
the
other
variables.
Also,
using
the
K
Matrix
method,
it
is
shown
which
method
of
treatment
(independent
variable)
has
had
a
greater
effect
on
the
dependent
variables.
The
test
assumptions,
including
the
homogeneity
of
regression,
linear
relationship,
homogeneity
of
variance
-
covariance
matrices
and
variances
equality
were
tested
and
all
were
confirmed.
Descriptive
findings
(descriptive
indicators
of
dependent
variables)
Table
1:
Mean
and
standard
deviation
of
the
pre-test
of
experimental
and
control
groups
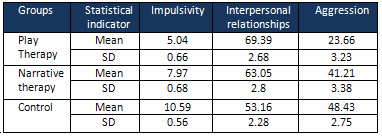
As
can
be
seen
in
[Table
1],
after
adjusting,
the
scores
of
experimental
and
control
groups
in
the
post-test
of
impulsivity,
interpersonal
relations
and
aggression
are
different
from
each
other.
To
examine
whether
this
difference
is
statistically
significant
or
not,
and
if
it
is
caused
by
the
effect
of
education,
the
MANCOVA
analysis
with
"Bonferroni"
correction
was
performed
by
K
Matrix
method.
Inferential
results
Table
2:
Testing
the
combined
effect
size
based
on
Wilks
Lambda
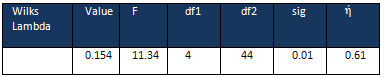
According
to
the
above
table
and
based
on
adjusted
Bonferroni
alpha
(0.017),
training
of
group
narrative
therapy
and
play
therapy
has
had
a
significant
effect
on
impulsivity,
aggression
and
interpersonal
relationships
in
a
composite
variable
with
?Partial
=
0.53,
Wilk's
Lambda
=
0.154
and
F
(44.4)
=
11.34
(P
<
0.01).
The
Eta
squares
values
seen
in
the
above
table
are
a
parabola
of
the
variance
related
to
the
new
composite
variable.
The
general
rule
implies
that
if
this
amount
is
greater
than
0.14,
the
size
effect
is
high.
The
Eta
parabola
square
shows
the
severity
of
this
effect
(0.61),
which
indicates
a
very
high
size
effect.
The
significant
effect
of
training
group
narrative
therapy
and
play
therapy
on
impulsivity,
aggression
and
interpersonal
relationships
indicates
that
the
means
of
dependent
variables
are
different
in
these
groups.
Table
3:
Testing
the
effectiveness
of
group
narrative
therapy
and
play
therapy
on
inhibiting
impulsivity,
reducing
aggression
and
increasing
interpersonal
relations
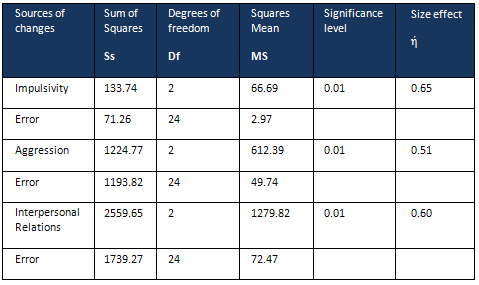
According
to
the
results
in
[Table
3]
and
based
on
adjusted
Bonferroni
alpha
(0.017),
the
effectiveness
of
group
narrative
therapy
and
play
therapy
to
inhibit
impulsivity
with
F
(2.24)
=
22.52,
the
effectiveness
of
group
narrative
therapy
and
play
therapy
in
reducing
aggression
with
F
(2.24)
=
12.31
and
the
effectiveness
of
group
narrative
therapy
and
play
therapy
on
increasing
the
interpersonal
relations
with
F
(2.24)
=
17.66
have
been
effective
(P
<
0.01).
To
accurately
examine
these
mean
differences,
the
results
of
multiple
comparison
test
(K
Matrix)
are
reported.
Table
4:
Examining
the
differences
of
effects
of
group
narrative
therapy
and
play
therapy
on
impulsivity,
aggression,
interpersonal
relations
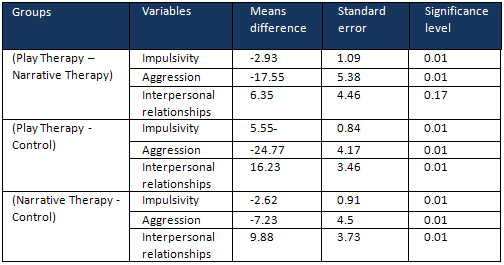
The
post
hoc
test
of
comparing
the
mean
effect
of
group
narrative
therapy
and
play
therapy
on
impulsivity
also
shows
that
the
mean
difference
(-2.93)
is
statistically
significant
(P
?
0.01).
Therefore,
one
can
conclude
that
the
effectiveness
of
group
play
therapy
training
on
impulsivity
is
different
from
narrative
therapy
effect,
and
group
play
therapy
has
more
affected
impulsivity
than
group
narrative
therapy.
The
post
hoc
test
to
compare
the
mean
effect
of
group
narrative
therapy
and
play
therapy
on
aggression
also
shows
that
the
mean
difference
(-17.55)
is
statistically
significant
(P
<
0.01).
Therefore,
one
can
conclude
that
the
effectiveness
of
group
play
therapy
training
on
aggression
is
different
from
narrative
therapy
effect,
and
group
play
therapy
has
more
affected
aggression
than
group
narrative
therapy.
The
post
hoc
test
to
compare
the
mean
effect
of
group
narrative
therapy
and
play
therapy
on
interpersonal
relations
also
shows
that
the
mean
difference
(6.35)
is
not
statistically
significant
(P
>
0.17).
Therefore,
one
can
conclude
that
the
effectiveness
of
group
play
therapy
training
on
interpersonal
relations
is
not
significantly
different
from
narrative
therapy
effect.
| DISCUSSION
AND
CONCLUSION
|
This
study
aimed
to
evaluate
and
compare
the
effectiveness
of
group
narrative
therapy
and
play
therapy
on
inhibiting
impulsivity,
reducing
aggression
and
increasing
interpersonal
relations.
The
main
hypothesis
was
to
investigate
whether
the
effectiveness
of
narrative
therapy
on
inhibiting
impulsivity,
reducing
aggression
and
increasing
interpersonal
relations
is
different
from
group
play
therapy
or
not.
Based
on
the
results,
we
can
conclude
that
the
play
therapy
method
has
been
more
effective
on
variables
of
impulsivity
and
aggression
in
comparison
with
narrative
therapy
method.
In
the
case
of
interpersonal
relationships
variable,
these
two
treatment
methods
are
not
significantly
different,
and
their
mean
differences
are
not
statistically
significant.
Thus,
to
reduce
symptoms
of
aggressive
behaviors
and
control
and
inhibition
of
impulsive
behaviors,
play
therapy
interventions
are
more
efficient
than
narrative
therapy
approach.
However,
in
the
case
of
interpersonal
relations
variable,
none
of
the
therapies
have
no
advantage
relative
to
each
other,
and
the
therapist
chooses
the
desired
treatment
method
based
on
the
diagnosis
provided
by
the
references.
The
results
of
this
study
are
consistent
with
the
findings
of
the
following
research:
Baggerly
and
Parker
studies
(2005)
based
on
the
effectiveness
of
child-centered
play
therapy
to
treat
the
problems
of
boys
in
primary
schools
[27],
Baggerly
research
(2012)
based
on
the
effectiveness
of
group
child-centered
play
therapy
on
self-esteem,
depression
and
anxiety
of
parentless
children
[28],
Lindau
et
al.
studies
(2012)
based
on
the
effectiveness
of
group
child-centered
play
therapy
on
attitudes,
knowledge
and
skills
of
students
[29],
Ray
Blanco
et
al.
study
(2009)
on
the
effectiveness
of
play
therapy
in
reducing
aggression
in
aggressive
children
[30],
Kristin
and
Mini
Whalen
et
al.
research
(2016)
based
on
the
effect
of
Adler
play
therapy
in
reducing
externalizing
behaviors
and
weak
social
skills
[31],
Rahmani
study
(2011)
based
on
the
effectiveness
of
storytelling
on
reducing
children's
reading
disorders
[32],
Hassani,
Farahbakhsh,
&
Shafiabadi
(2015)
based
on
the
effectiveness
of
narrative
therapy
on
reducing
behavioral
disorders
in
adolescents
[33],
Onyut
et
al.
studies
(2015)
based
on
the
reduction
of
PTSD
symptoms
due
to
war
with
play
therapy
[34],
finally,
Farzadfarz,
Abdekhodaee
&
Ghenaeechaman
Abadi
research
(2015)
based
on
the
effectiveness
of
narrative
therapy
and
play
therapy
on
increasing
attention
and
focus
of
children
[35].
In
general,
play
therapy
and
storytelling
have
been
effective
in
reducing
the
symptoms
of
aggression,
impulsivity
and
increasing
skills
in
interpersonal
relationships.
Stories
and
plays
provide
time
for
excitement
release
and
refinement
and
adjustment
of
trill
.
These
variables
have
been
effective
in
reducing
aggression
and
impulse
control
power
in
children.
Also,
narrative
and
play
therapies
improve
communication
skills
and
interpersonal
and
intrapersonal
relations,
and
affect
the
individual
behaviors
covertly
and
overtly.
In
storytelling,
children's
become
sympathetic
with
the
tale
characters.
These
characters
are
suitable
models
for
children,
which
lead
to
increased
self-confidence
and
externalizing
positive
and
negative
emotions.
Regarding
the
difference
between
group
storytelling
and
play
therapy,
one
can
say
that
the
participation
of
children
in
the
process
of
playing
was
more
than
storytelling,
the
play
therapist
has
well
performed
practices
such
as
dough
playing
and
playing
with
small
animals
fitted
to
the
children's
interests,
and
the
diversity
and
participation
rate
have
been
effective
in
these
interactions.
Based
on
the
results,
it
is
suggested
to
use
group
play
therapy
approaches
in
the
treatment
of
aggressive
and
impulsive
children.
In
addition,
the
counselors
and
psychotherapists
are
recommended
to
use
both
narrative
therapy
and
play
therapy
techniques
for
increasing
self-confidence
and
improving
and
increasing
interpersonal
relationships.
It
is
suggested
to
conduct
this
study
on
male
and
female
subjects
and
compare
them
with
each
other.
The
results
can
be
also
used
in
treatment
of
children
with
psychological
disorders
such
as
conduct
disorder
and
oppositional
defiance
disorder.
1-
Asghari
Nekah,
M.,
&
Barook,
M.
(2016).
Examining
the
effectiveness
of
intervention
based
on
linguistic
games
on
the
development
of
phonological
awareness
of
parentless
children
and
children
with
irresponsible
caretakers
residing
in
nursery.
Research
in
clinical
psychology
and
counseling,
5
(1),
86-100.
2-
Aslipoor
A.,
Kafie,
M.,
&
Khosro
javid,
M.
(2013).
Applying
appearance
test
to
comparing,
Psychological
characteristics
of
foster
student
abnormal
in
families.
Journal
Faslname
Mehrschool
Psychology,
2
(5)
6-22.
3-
Hesarsorkhi,
R,
Tabibi,
Z,
Asghari-Nekah,
S,
Bagheri,
N.
Effectiveness
of
Emotional
Competence
Training
on
Improving
Emotional
Knowledge,
Emotional
Regulation
and
Decreasing
Aggression
in
Orphans
and
Abandoned
Children.
Journal
of
Clinical
Psycology,3.
2016;
8
(3):37-48
4-
Khazaie
H,
Asadi
M,
Mohammadi
H.
Influence
of
reinforcement
behavioral
therapy
and
Ellis
cognitive
therapy
on
derelict
children's
aggression.
Journal
of
Kermanshah
University
of
Medical
Sciences
(J
Kermanshah
Univ
Med
Sci).
2012
Mar
2;15(6).
5-
Longa,
C.
(2011)
Social
aggression
in
children
and
adolescents;
A
meta-analytic
review
(doctoral
dissertation).
Open
access
dissertation.625.
6-
Kennedy-behr,
A.,
Rodger,
S.,
&
Mickan,
S.
(2013).
Aggressive
interaction
during
free-play
at
preschool
of
children
with
and
without
developmental
coordination
disorder.
British
Journal
of
Occupational
therapy,
74
(7)
.348-354.
7-
Bas,
A.U.,
&
Kabasakal,
Z.T.
(2010).
Teachers
view
and
knowledge
about
reactive
and
proactive
aggression.
Procedia
social
and
Behavioral
science,
2,
1564-1580.
8-
Ekhtiari,
M.,
Rezvanfard,
M.,
&
Mokri,
A.
(2009).
Impulsivity
and
its
various
assessment
tools:
Review
of
views
and
studies.
Journal
of
Psychiatry
and
Psychology,
14(3),
247-257.
9-
Pico,
B.
P.
(2014).
Impulsivity
depression
and
aggression
among
adolescent.
Personality
and
Individual
Differences.
Am
J
Psychiatry,69.33-37.
10-
Burton,
C.
L.,
&
Fletcher,
P.
J.
(2012).
Age
and
sex
difference
in
impulsive
action
in
rats:
the
role
of
dopamine
and
glutamate.
Behavioral
Brain
Research,
230,
21-30.
11-
Carlotta,
D.,
Borroni,
S.,
Maffei,
C.,
&
Fossati,
A.
(2011).
The
role
of
impulsivity,
sensation
seeking
and
aggression
in
the
relationship
between
childhood
AD/HD
symptom
and
antisocial
behavior
in
adolescence.
Neurology,
Psychiatry
and
brain
research,
17(4),
89-98.
12-
Kowalski,
R.
M.,
&
Fedina,
C.
(2011).
Cyber
bullying
in
ADHD
and
Asperger
Syndrome
population.
Research
in
Autism
Spectrum
Disorders.5,
1201-1208.
13-
Wike,
T.
L.
(2011).
The
Effectiveness
of
a
Social
Skills
Intervention
for
Preventing
Aggression
in
Children:
An
Evaluation
of
the
Making
Choices
Intervention.
14-
Heydari,
M.
(2012).
The
effectiveness
of
early
childhood
education
on
social
skills
of
primary
school
children;
MA
Thesis
of
Education
Sciences,
Payam
Noor
University,
Faculty
of
Humanities.
15-
Glover
NM.
Play
therapy
and
art
therapy
for
substance
abuse
clients
who
have
a
history
of
incest
victimization.
Journal
of
Substance
Abuse
Treatment.
1999
Jun
30;16(4):281-7.
16-
Axline
VM.
Play
therapy.
Ballantine
Books;
2012
Feb
8.
17-
Landreth,
G
.L.
(2002).
Play
therapy:
The
art
of
the
relationship.
New
York:
Brunner
Routledge.
18-
Nasirzadeh,
R.,
&
Roshan,
R.,
(2011);
Effectiveness
of
storytelling
on
reducing
aggression
in
6
to
8
years
old
boys.
Iranian
Journal
of
Psychiatry
and
Clinical
Psychology,6(2),
118-126.
19-
Desocio.
J.
E.
(2005).
Assessing
self-development
through
Narrative
approaches
in
child
and
adolescent
Psycho
Therapy.
Journal
of
Child
and
Adolescent
Psychiatric
Nursing,
18,
53-61.
20-
Asghari
Nekah,
M.,
&
Barook,
M.
(2016).
Examining
the
effectiveness
of
intervention
based
on
linguistic
games
on
the
development
of
phonological
awareness
of
parentless
children
and
children
with
irresponsible
caretakers
residing
in
nursery.
Research
in
clinical
psychology
and
counseling,
5
(1),
86-100.
21-
Galdard,
K.,
&
Galdard,
K.
(2003).
A
practical
guide
in
consultation
with
children;
Translation:
Parniani,
Mino
(2004),
Tehran,
Roshd
Publication
22-
Landreth
GL.
Innovations
in
play
therapy.
Routledge;
2013
Jun
17.
23-
French
DC,
Jansen
EA,
Pidada
S.
United
States
and
Indonesian
children's
and
adolescents'
reports
of
relational
aggression
by
disliked
peers.
Child
development.
2002
Jul
1;73(4):1143-50.
24-
Shahim
S,
Yosefi
F.
The
questionnaire
of
preschool
children
behavioral
difficulties
parental
form.
J
Human
and
Social
Sciences
2000;
15
(1):
1-14.
25-
Saati,
S.,
(2016).
Validation
of
Gestalt
Bandar
in
the
components
of
aggression,
impulsivity
and
anxiety
in
schoolchildren.
Master's
thesis
in
clinical
psychology.
Rasht
Islamic
Azad
University,
Faculty
of
Humanities
26-
Hossienchari,
M.
(2008).
Compare
perceived
self-efficacy
in
social
interaction
with
peers
in
a
group
of
and
girl
and
boys
students.
Psychological
Studies,
3,
4,
87-103
27-
Baggerly,
J.,
&
Parker,
M.
(2005).
Child-centered
group
play
therapy
with
African
American
boys
of
the
elementary
school
level.
Journal
of
Counseling
Developmental,
83,
387-396.
28-
Baggerly,
J.
(2012).
The
effects
of
child-
center
group
play
therapy
on
self-concept,
Depression
and
Anxiety
of
Children
who
are
homeless.
International
Journal
of
Play
Therapy,
13
(2):
31-51.
29-
Lindo,
N.
A.,
Chung,
C.
F.,
Carlson,
S.,
Sullivan,
J.
M.,
Akay,
S.,
&
Meany-Walen,
K.
K.
(2012).
The
impact
of
child-centered
play
therapy
training
on
attitude,
knowledge,
and
skills.
International
Journal
of
Play
Therapy,
21(3),
149.
30-
Ray,
D.
C.,
Blanco,
P.
J.,
Sullivan,
J.
M.,
&
Holliman,
R.
(2009).
An
exploratory
study
of
child-centered
play
therapy
with
aggressive
children.
International
Journal
of
Play
Therapy,
18(3),
162.
31-
Meany-Walen
KK,
Teeling
S.
Adlerian
play
therapy
with
students
with
externalizing
behaviors
and
poor
social
skills.
International
Journal
of
Play
Therapy.
2016
Apr;25(2):64.
32-
Rahmani,
P.
(2011).
The
efficacy
of
narrative
therapy
and
storytelling
in
reducing
reading
errors
of
dyslexic
children.
Procedia-Social
and
Behavioral
Sciences,
29,
780-785.
33-
Hassani,
A.
Frhbkhsh,
K.
Shafiabadi,
AS.
(2015).
To
evaluate
the
effectiveness
of
cognitive-behavioral
story
and
narrative
therapy
on
reducing
behavioral
disorders
in
adolescents.
Research
in
Clinical
Psychology
and
Counseling,
4
(1),
94-71.
34-
Onyut
LP,
Neuner
F,
Schauer
E,
Ertl
V,
Odenwald
M,
Schauer
M,
Elbert
T,
(2005).
Narrative
Exposure
Therapy
as
a
treatment
for
child
war
survivors
with
posttraumatic
stress
disorder:
Two
case
reports
and
a
pilot
study
I
an
African
refugee
settlement.
BMC
Psychiatry,
5:
7.
35-
Farzadfard,
S.
A.,
Abdekhodaee,
M.
S.,
&
Ghenaeechaman
Abadi,
A.
(2015).
Effectiveness
Of
Combined
Purposeful
Play
therapy
and
narrative
therapy
on
Pre-school
children's
attention
and
concentration.
Journal
of
Fundamentals
of
Mental
Health.17
(5),
22-28.
|

