|
Self-monitoring of Blood Glucose
Among Type-2 Diabetic Patients: An Analytical
Cross-Sectional Study
Ahmed S. Alzahrani
(1)
Rishi K. Bharti (2)
Hassan M. Al-musa (3)
Shweta Chaudhary (4)
(1) Family Medicine specialist, Community medicine
resident, Abha, King Khalid University Saudi
Arabia
(2) Assistant Professor, Community medicine
consultant, Faculty of Medicine, King Khalid
University,
Saudi Arabia.
(3) Associate Professor, Family Medicine consultant,
Family and Community medicine department,
Faculty of medicine, King Khalid University,
Saudi Arabia.
(4) Assistant Professor, Department of Anatomy,
Faculty of Medicine, King Khalid University,
Saudi Arabia.
Corresponding
author:
Dr. Ahmed
Salem Al-zahrani,
Family Medicine specialist, Community Medicine
resident
Abha, King Khalid University, Saudi Arabia
Email : ahmedalzahrani122333@gmail.com
|
Abstract
Background: Diabetes mellitus (DM)
is a public health disease needing urgent
consideration; it has a great impact on
human life in addition to being costly
to manage. According to the current recommendations,
self-monitoring of blood glucose (SMBG)
is important in order to achieve and maintain
glycemic control, prevent and identify
hypoglycemia, prevent severe hyperglycemia
and support lifestyle changes.
Methods: The objective of this
study is to explore the effect of using
SMBG on glycemic control among type 2
diabetic patients attending the primary
health care centers in Abha city in the
Kingdom of Saudi Arabia, by comparing
those who are monitoring themselves and
others who are not. The study design was
analytical cross-sectional and conducted
through an interviewing questionnaire.
Results: The age of participants
was 30-82 years old, with a mean age distribution
of 57.4 years old. The percentages of
groups doing and not doing SMBG were 43%
and 57% respectively. Chi square tests
show that the relationship between glycemic
control and SMBG is statistically significant
according to frequency and time of doing
SMBG, since almost all of the results
for the participants who do SMBG are above
the target for glycemic control (>=7%).
The relationship between glycemic control
and compliance according to SMBG shows
there is a statistically significant relationship
with appointment compliance among the
group doing SMBG, and with drug compliance
among the other group.
In both groups, almost all the participants
were above the target for control (>=7%),
which means that there is no relationship
between doing SMBG and better glycemic
control.
Conclusion:
There is not sufficient evidence to
show that the self-monitoring of blood
glucose is associated with an improvement
in glycemic control among type 2 diabetics
and it is shown that glycemic control
for both groups that are using and not
using SMBG is above the target. It is
recommended that more well conducted randomized
controlled trials should be undertaken
to evaluate the relationship between SMBG
and glycemic control in type 2 diabetes,
at the same time the current guidelines
for the use of SMBG among patients with
well controlled non-insulin treated type
2 diabetes need to be reviewed.
Key words: Self-monitoring, blood
glucose (SMBG), glycemic control, type
2 diabetes, comorbidities.
|
Diabetes mellitus is a group of metabolic diseases
characterized by hyperglycemia that results
from defects in insulin secretion, action or
both(1).
Diabetes can be classified into type 1 diabetes
(B-cell destruction usually leading to absolute
insulin deficiency), type 2 diabetes (ranging
from being characterized predominantly by insulin
resistance with relative insulin deficiency
to predominantly an insulin secretory defect
with insulin resistance) and other specific
types of diabetes (1).
Diabetes and its complications are major causes
of death in many countries. Type 2 is the most
prevalent type occurring in up to 91% of adults
with diabetes in high-income countries. It is
estimated that 193 million people with diabetes
are undiagnosed and they are more at risk of
developing complications (2).
The prevalence of type 2 diabetes in Saudi Arabia
is about 32.8%; the predicted prevalence will
be 35.37% in 2020; 40.37% in 2025 and 45.36%
in the year 2030. The coefficient on time factor
indicates that the prevalence rate has increased
from 1982-2015 (3).
Saudi Arabia should include preventive measures
against diabetes on a war footing basis in its
national health policy to minimise the burden
of the disease (3).
In patients with type 2 diabetes, SMBG can help
to achieve better glycemic control, although
there is not sufficient evidence to confirm
that strict monitoring in these patients is
associated with an improved outcome (4).
The outcome of several clinical studies, especially
amongst diabetics on insulin therapy, has shown
that SMBG plays a key role in preventing complications
in the short, medium and long term.
According to the American Diabetes Association
(ADA) and the National Academy of Clinical Biochemistry
(NACB), patients and healthcare personnel should
be trained on the appropriate use of the device,
as well as on the correct interpretation of
data (5).
In type 2 diabetes, the efficacy of frequent
glucose measurements remains uncertain. The
results of studies suggest that SMBG can play
an important role in improving metabolic control
if it is an integral part of a wider educational
strategy (6).
Higher SMBG testing rates were associated with
lower HbA1c, only when stratifying the analyses
to control for treatment intensification (4).
A significant reduction in HbA1c levels was
associated with Asian populations, in a small
sample size, and telecare, and with those patients
with baseline HbA1c greater than 8.0% (7).
There was no convincing evidence to support
a recommendation for routine self- monitoring
of all patients and no evidence of improved
glycemic control in predefined subgroups of
patients(8).
SMBG indications can be used as a measure for
acute correction ("primary adjustment"),
if blood glucose levels are increased or decreased
during intensive insulin therapy, when correction
may be made with rapid-acting insulin or administration
of carbohydrate (9).
The OneTouch® Select Simple™ glucose
meter meets current regulatory expectations
for glucose meter performance (10) and consideration
of personal aspects of daily living that impact
on an individual's ability to achieve their
desired glycemic control(11).
Optimal glycemic control will improve long-term
outcomes in many patients with diabetes. Tools
such as new therapeutics and advanced technology,
including highly accurate BGMSs, will help patients,
working alongside their diabetes teams, to achieve
the goal of improved glucose control (12).
The health burden due to DM in Saudi Arabia
is predicted to rise to catastrophic levels,
unless a wide-ranging epidemic control program
is adopted, with great emphasis on healthy diet,
including exercise and active lifestyles, and
weight control. To properly manage DM in Saudi
Arabia, a multidisciplinary approach is required
(13).
SMBG is recommended as an essential part of
daily DM management regardless of type and mode
of treatment strategy of adjusting medication
at monthly intervals based on intensified SMBG
data can be adopted in conjunction with HbA1c
results to achieve better glycemic control (14).
According to one published study, 15.3% of people
with type 2 diabetes practice SMBG (15).
Results of a Saudi study conclude that SMBG
has a positive impact on glycemic control, expressed
as decrease in HbA1c levels with time post referral(19).
T2DM patients following SMBG have shown better
lifestyle changes and compliance to drug therapy.
It could be due to regular monitoring of blood
glucose levels thereby patients became motivated
and understood the importance of dietary changes,
regular exercise and intake of antidiabetic
pills in controlling the disease and its associated
complications(19). Patients following SMBG have
also shown a more positive attitude and awareness
about diabetes and risk factors associated with
it than patients without SMBG follow-up (19).
According to ADA, the glycemic targets are :
HBA1c at target (defined as <7%) and not
at target (defined as >7) (19).
FBS at target (defined as 80-130mg/dl) and not
at target (defined as >130mg/dl) (20). RBG
at target (defined as <180 mg/dl.) and not
at target (defined as >180mg/dl) (20).
This study aimed to explore the effect of using
SMBG on glycemic control among type 2 diabetic
patients at Abha city's PHCCs.
This
research
had
an
analytical
cross-sectional
study
design
to
explore
the
effect
of
SMBG
on
glycemic
control
among
type
2
diabetics
in
Abha
city's
PHCCs
by
comparing
those
who
are
doing
it
and
others
who
are
not
doing
it.
Type
2
diabetic
patients
attending
governmental
primary
health
care
centres
(PHCCs),
excluding
those
with
type
1
and
gestational
diabetes,
made
up
the
study
population.
There
are
about
10
primary
health
care
centres
in
Abha
city
according
to
Abha
sector
of
Aseer
health
affairs,
serving
about
5,000
diabetic
patients.
The
study
used
STATCALC
EPI
software
and
the
sample
size
was
314
calculated.
The
sample
was
recruited
using
systematic
random
sampling
of
patients
attending
the
PHC.
The
data
were
collected
using
a
validated
questionnaire
which
was
distributed
and
initiated
through
an
interview
with
participants.
The
study
was
approved
by
the
ethical
committee
(institutional
review
board),
and
permission
was
granted
by
Aseer
health
affairs.
Consent
was
obtained
from
participants
verbally.
Data
were
cleaned,
coded,
entered
and
analyzed
using
SPSS
version
21.
Participants
were
aged
between
30
and
82
years
old
with
a
mean
age
distribution
of
57.4.
Males
constituted
47.8%
of
the
sample
and
females
made
up
52.2%.
The
bio-demographic
characteristics
of
type
2
diabetic
patients
according
to
their
self-monitoring
of
blood
glucose
status
are
shown
in
Table
1.
Click
here
for
Table
1:
Bio-demographic
characteristics
of
type
2
diabetic
patients
according
to
their
self-monitoring
of
blood
glucose
status
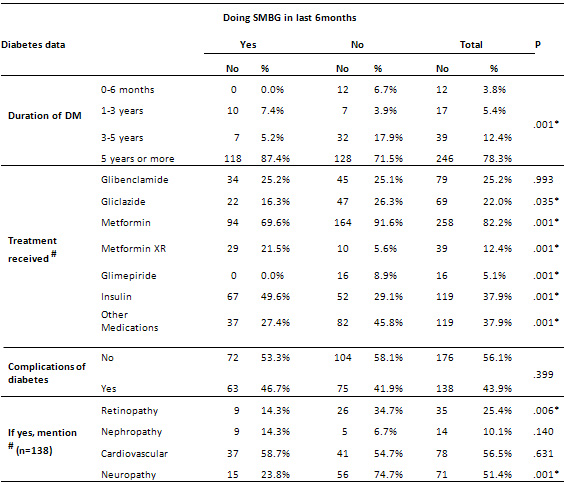
Table
2
reveals
complications
of
diabetes
were
present
in
about
43.9%
of
the
participants
(46.7%
among
the
group
doing
SMBG)
with
25.4%
Retinopathy
(14.3%
were
doing
SMBG
and
34.7
were
not),
Neuropathy
is
about
51.4%
(23.8%
were
doing
SMBG
and
about
74%
were
not).
About
78.3
%
of
participants
had
diabetes
for
five
years
or
more
(87.4%
among
those
doing
SMBG),
the
majority
of
treatment
received
was
by
metformin
in
about
82.2%
of
participants:
69.6%
were
doing
SMBG
and
91.6%
were
not;
the
lowest
is
glimepiride
by
5.1%.
Comorbidities
of
diabetes
were
present
in
51.3%
of
all
participants:
hypertension
50%,
lipid
disorders
26%,
obesity
4%
and
others
20%.
Click
here
for
Table
2:
Diabetes
data
for
patients
according
to
their
self-monitoring
of
blood
glucose
status
In
the
group
doing
SMBG:
46%
had
comorbidities
and
54%
had
no
comorbidities,
while
in
the
other
group:
55%
had
comorbidities
and
45%
had
no
comorbidities.
Our
result
shows,
causes
of
not
doing
SMBG
were
mainly
because
of
unavailability
of
strips
(36%)
and
no
desire
(about
24%).
Table
3
shows
the
number
of
people
doing
SMBG
three
times
a
day
was
lowest
at
5.2%,
and
twice
a
day
was
highest
at
45.9%,
and
moderately
more
than
once
a
week
by
about
25%.
Time
of
doing
SMBG
was
before
meals
in
59.3%,
feeling
of
hypoglycemic
episode
35.6%
and
during
episode
of
illness
5.2%.
The
scale
of
was
SMBG
helpful
shows
extremely
helpful
in
28.9%,
somewhat
helpful
in
40.7%,
slightly
helpful
in
11.9%
and
not
at
all
helpful
in
0.7%.
For
reason
for
SMBG
being
helpful
if
scale
was
7
or
more
it
indicated
the
following:
improved
diabetes
control
(70.0%),
help
during
episode
of
illness
(12.7%),
better
to
do
physical
activity
(9.1%)
and
avoid
hypoglycemia
(8.
Reason
for
SMBG
being
helpful
if
scale
is
4
or
less
is
because
it
is
painful
100%.
Good
diet
compliance
constitutes
about
28
%,
fair
55%
and
poor
18
percent.
Good
drug
compliance
constitutes
about
54
percent,
fair
45%
and
poor
about
0.64%.
Diet
compliance
among
the
group
doing
SMBG
was
fair
(54.1%),
good
(40%)
and
poor
(10%).
Drug
compliance
among
them
was
fair
(29%),
good
(70%)
and
poor
(1.5%),
Physical
activity
compliance:
fair
in
63%,
good
in
24%
and
poor
in
13%
appointment
compliance:
fair
in
38%,
good
in
61%
and
poor
in
0.7%.
Click
here
for
Table
3:
Relationship
between
glycemic
control
and
SMBG
among
type
2
diabetic
patients
Table
4
shows
the
relationship
between
glycemic
control
and
SMBG:
In
relation
to
glycemic
control
the
frequency
of
SMBG
once
daily
was
in
26%
at
target,
once
a
week
in
46%
while
twice
a
day,
three
times
a
day
and
more
than
once
a
week
all
were
not
at
target
100%.
Time
of
doing
before
meals
was
at
target
in
14%
while
during
episode
of
illness
and
feeling
of
hypoglycemic
episode
was
not
at
target
100%.
Not
all
scales
of
'helpful'
were
at
target
except
extremely
helpful
15%
and
somewhat
helpful
9%
were
at
target.
Findings
elicit
the
relationship
between
glycemic
control
and
compliance
according
to
SMBG:
among
the
group
of
doing
SMBG:
diet
compliance
was
good
and
at
target
in
9%,
fair
and
at
target
in
8%
and
poor
and
at
target
0%
drug
compliance:
good
and
at
target
in
12%,
fair,
poor
and
at
target
in
0%.
Physical
activity
compliance:
good
and
at
target
in
16%,
fair
and
at
target
in
7%
and
0
in
poor,
Appointment
compliance:
good
and
at
target
13%,
fair,
poor
and
at
target
0%.
Click
here
for
Table
4:
Relation
between
glycemic
control
and
compliance
according
to
SMBG
among
type
II
diabetic
patients
Findings
show
that
about
57%
are
not
doing
SMBG
in
last
6
months
and
only
43%
are
not
doing
SMBG
in
last
6
months
and
only
43%
are
doing
it.
|


{kind=link}