|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
|
|
|
|
........................................................
|
Original
Contribution/Clinical Investigation
|
|
|
<-- Turkey -->
Preoperative
management of sickle cell patients with hydroxyurea
[pdf version]
Mehmet Rami Helvaci,
Sedat Hakimoglu, Mehmet Oktay Sariosmanoglu,
Suleyman Kardas, Beray Bahar, Merve Filoglu,
Ibrahim Ugur Deler, Duygu Alime Almali, Ozcan
Gokpinar, Ozlem Celik, Aynur Ozbay, Ozgun Ilke
Karagoz, Seher Aydin
<-- Ethiopia-->
Khat
(Catha edulis) chewing as a risk factor of low
birth weight among full term Newborns: A systematic
review
[pdf version]
Kalkidan Hassen
<-- Australia -->
Chronic
pain review following Lichtenstein hernia repair:
A Personal Series
[pdf
version]
Maurice Brygel,
Luke Bonato, Sam Farah
<-- Saudi Arabia -->
Assessment
of Health Status of Male Teachers in Abha City,
Saudi Arabia
[pdf
version]
Ali Mofareh Assiri,
Hassan M. A. Al-Musa
|
|
........................................................ |
Evidence
Based Medicine
........................................................
Medicine and Society
........................................................
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| October 2015 -
Volume 13 Issue 7 |
|
|
Assessment of Health
Status of Male Teachers in Abha City, Saudi
Arabia
Ali
Mofareh Assiri (1)
Hassan M. A. Al-Musa (2)
(1) MB BS, Saudi Board of Family Medicine
(2) MB BS, ABFM, Consultant & Associate
Professor
Chairman, Family and Community Medicine Department
College of Medicine, King Khalid University
Correspondence:
Dr. Hassan M. A. Al-Musa
Family and Community Medicine Department
College of Medicine,
King Khalid University
P.O. Box 641, Abha, K.S.A
Contact No.: 0501882929
Email: fcmcomkku@gmail.com;
almusa3@hotmail.com
|
Summary
This study was
done to assess the health aspect of male
teachers (384) and to assess level of
job satisfaction of male teachers in different
grades in Abha city.
Following a simple random sample, the
sample from primary 184 (47.9%), intermediate
132 (34.4%) and secondary 68 (17.7%) school's
male teachers in Abha City were selected.
All respondent teachers were exposed to
the validated questionnaire to assess
health problem [medical history and co-morbidities]
and work place risk factors.
The background data as age was 39.31 ±7.96[23:75]
years; the average experience years were
16.1 ±7.43[1:36] years and 71.6%
have experience more than 10 years. 100
% of the sample were males due to socio-cultural
matters, as regard to the educational
level 47.9% were from primary schools,
34.4% from intermediate schools and 17.7%
from secondary schools.
The level of satisfaction regarding current
job and salary of teachers revealed that
65.6% were satisfied while 34.4% were
not satisfied.
The answers about some medical history
like history of having medical problems
that affect teacher's ability (9.4%),
history of treatment in hospital (25.5%)
, sick leave 19% and all were within accepted
range, apart from seeing a doctor in last
year (43.2%).
The complaints or health problems among
teachers as regards eyesight problems
15.4%, Hearing problems in 6.5%, Mental
illness, psychological or psychiatric
problem was 7.8%. The history of drug
or alcohol problem was 2.3%, skin problems
12%, history of hepatitis or jaundice
1.6%. The heart or blood pressure problems
were 11.32%. The history of allergies
was 17.4%; asthma or chest problem was
reported in 20.8% and cough for more than
3 weeks, coughed up blood or had any unexplained
weight loss or fever, was 9.6%.
The history of Musculoskeletal disorders
(MSD) was 21.1%, Low back pain (LBP) 21.6%
and joint pain 32%. Regarding feeling
well and healthy 154 (32%) gave the answer
that they are NOT healthy or feeling well.
The relation between ill health and experience
years gave a significant association but
no significant association with teaching
level.
The relation between job satisfaction
and experience years showed no significant
difference with experience years, but
the higher rates with longer experience
(70.2%) and gave significant relation
with level especially at primary level.
|
Teachers' work today is multifaceted as they
undertake not only teaching but also matters
associated with curriculum, students, parents,
the school community and departmental initiatives
[1].
These are tough times to be a teacher. Emerging
issues of concern in the teaching profession
are attrition rates and burnout levels. Ewing
and Smith [2] reported that between 25% and
40% of beginning teachers in countries in the
Western World are leaving teaching or they are
burned out.
In Australia, a study [3] highlighted an upward
trend in early-career teacher resignations and
according to Macdonald [4] overall teacher attrition
in Australian government schools ranges from
3% to 8%. When this is considered in conjunction
with the impending teacher shortage in Australia
[5], it is important to determine how teachers
feel about their roles as this has implications
for meeting society's expectations for education
and for youth today; it also has implications
for teacher well-being.
Well-being, according to Dunn [6] involves comparative
private experiences with regard to self-perceived
quality of an individual's life; it also includes
both affective and cognitive components.
Factors that influence teacher well-being,
burnout and competence
Traditionally, the role of teaching has been
one of nurturing and developing students' potential;
teachers play a valuable role in helping children
grow. In order to do this they must remain physically
and mentally well [7]. However, there is apparent
dissonance between teachers' perceived capacities
and the expectations of their role. This may
have implications for their physical and mental
well-being and their professional competence
as teachers [8].
Teacher well-being and competence have been
related to job satisfaction and studies indicate
that those teachers who are less satisfied are
more likely to leave teaching. For example,
Singh and Billingsley [9] found factors such
as stress, burnout, work overload, and job dissatisfaction
contribute to teacher attrition while factors
such as administrative support, reasonable role
expectations, and decreased workplace stress
contribute to teachers' intention to stay in
teaching. Principals play a pivotal role in
steering the direction of their school which
requires guiding the day-to-day business of
the school including matters associated with
both students and teachers.
The Management of Health and Safety at Work
Regulations 1999 addressed various health hazards
to which teachers are exposed [10].
Fitness criteria
To be able to undertake teaching duties safely
and effectively, it is essential that individual
teachers: have the health and well-being necessary
to deal with the specific types of teaching
and associated duties (adjusted, as appropriate)
in which they are engaged; are able to communicate
effectively with children, parents and colleagues;
possess sound judgment and insight; remain alert
at all times; can respond to pupils' needs rapidly
and effectively; are able to manage classes
and do not constitute any risk to the health,
safety or well-being of children in their care.
Where disabilities exist, teachers should be
enabled by reasonable adjustments, to meet these
criteria. The decision on fitness should be
considered using the above criteria and should
be based on an individual's ability to satisfy
those criteria in relation to all duties undertaken
as part of their specific post and in relation
to all of the individual's health problems [11]
Saudi
Arabia
is
a
country
with
an
independent
monarchy
situated
in
South
West
Asia.
The
first
feature
of
the
educational
system
in
Saudi
Arabia
is
the
combination
of
different
international
education
systems
along
Islamic
lines.
The
Ministry
of
Education
(MOE)
was
founded
in
1954
as
a
replacement
to
the
Directory
of
Education.
It
is
the
responsible
body
for
educational
policy
development
of
the
curriculum
and
teaching
methods.
The
educational
system
is
highly
centralized,
and
decision
making
is
top-down.
General
education
is
divided
into
three
main
levels:
primary
level
for
six
years,
middle
level
for
three
years
and
secondary
level
for
three
years.
The
schools
in
each
city
of
Saudi
Arabia
come
under
the
responsibility
and
supervision
of
the
Educational
Administration
[12].
Due
to
the
importance
of
Education
in
the
Socio-Economic
development
of
an
individual,
great
efforts
are
always
made
to
ensure
that
an
individual
goes
through
the
Education
cycle
successfully
by
achieving
high
academic
results.
The
need
for
good
results
puts
every
stake-holder
in
the
Education
Sector
on
alert.
Many
mechanisms
are
put
in
place
to
ensure
high
performance
and
good
results.
Such
mechanisms
include:
introducing
performance
contracts
by
the
government,
initiation
of
Free
Primary
Education
(FPE)
and
Subsidizing
Secondary
Education
(SSE),
increasing
contact
hours
between
the
teacher
and
learner,
holiday
tuition,
remedial
teaching
during
weekends,
intensive
testing
policies
[13].
In
considering
implications
of
health
problems
for
an
individual's
fitness
to
teach,
it
is
important
to
recognize
that
some
teaching
duties
involve
exposure
to
potential
health
hazards.
The
risk
arising
from
such
hazards
will
vary
according
to
the
specific
nature
of
the
teaching
duties
and
the
environment
in
which
the
teacher
is
working.
Teacher
training
providers
and
employing
organizations
have
a
statutory
responsibility
to
safeguard
the
health,
safety
and
welfare
of
teachers,
to
conduct
risk
assessments
and
take
steps
to
address
potential
hazards
and
reduce
the
risk
of
adverse
health
effects.
Occupational
health
professionals
have
a
key
role
in
advising
organizations
in
this
regard
[10].
Physical,
Chemical,
Biological
Teachers
are
potentially
exposed
to
a
range
of
physical,
chemical
and
biological
hazards.
The
following
are
examples:
Chemicals,
plant
and
animal
substances
in
those
teaching
the
sciences,
wood
dusts,
metal
fumes,
glues
and
noise
in
teachers
of
technical
subjects,
physical
violence
from
pupils
or
parents,
communicable
diseases,
ergonomic
problems
associated
with
bending,
manual
handling
and
sitting
on
small
chairs,
trauma
for
those
involved
in
teaching
physical
education
and
any
extra-curricular
activities
and
voice
trauma
[14].
Physical
Health
Only
a
few
studies
of
varying
quality
have
been
published
on
teachers'
physical
health.
When
considering
the
main
classes
of
diagnoses
of
physical
diseases;
musculoskeletal,
respiratory,
cardiovascular,
nervous
and
hormonal
disorders
[14].
Moreover,
when
focusing
on
cardiovascular
disorders,
a
study
carried
out
in
Germany
showed
that
there
was
a
lower
risk
for
male
teachers
compared
to
men
working
in
12
other
professions
[15].
Another
study
at
KSA
during
1995
found
the
prevalence
of
obesity
in
males
as
46%
and
females
49%
[16].
About
12%
of
all
teachers
were
considered
hypertensive,
18%
of
males
and
2%
of
females
were
current
cigarette
smokers.
A
greater
proportion
of
males
(57%)
than
females
(20%)
indicated
they
were
performing
a
physical
exercise
at
least
one
hour
per
week,
13%
of
males
and
11%
of
females
had
hypercholesterolemia.
Hypertriglyceridemia
was
found
in
12%
of
males
and
4%
of
females,
and
hyperglycemia
was
found
in
8%
of
males
and
4%
of
females.
Conclusions:
The
prevalence
of
cardiovascular
risk
factors
among
school
teachers
is
not
much
different
to
that
found
in
developed
countries
[16].
A
study
at
KSA
during
2006/2007
found
the
prevalence
of
hypertension
(HTN)
and
pre-hypertension
was
25.2
%
in
males
and
43.0
%
in
females
and
diabetes
was
significantly
associated
with
HTN
[17].
A
study
conducted
in
Sofia
,
Bulgaria
(1994),
found
that
the
estimated
relative
risk
of
arterial
HTN
for
female
teachers
was
1.5
compared
with
other
female
employees
(designers,
researchers)
who
served
as
controls.
This
finding
can
classify
the
teaching
occupation
as
high
risk
for
arterial
hypertension
[18].
MSD
represents
one
of
the
most
common
and
most
expensive
occupational
health
problems
in
both
developed
and
non-developing
countries
[19].
MSD
is
one
of
the
leading
causes
for
ill
health
retirement
among
school
teachers
[20].
Musculoskeletal
complaints,
especially
of
the
lower
back,
neck
and
shoulders
are
also
common
among
teachers.
Recently,
Hong
Kong
teachers
showed
a
higher
prevalence
for
neck
(68.9%),
shoulder
(73.4%)
and
low
back
pain
(59.2%)
in
the
past
30
days
[21].
Epidemiological
studies
have
demonstrated
that
factors
such
as
gender,
age,
length
of
employment
and
awkward
posture
are
associated
with
higher
MSD
prevalence
among
teachers
[19].
Among
workers
including
teachers,
prolonged
posture,
static
work
and
repetition
are
the
cause
of
repetitive
strain
injuries
(RSIs),
which
is
one
type
of
MSD
that
directly
affects
the
area
of
upper
limb,
neck,
shoulder
and
low
back
[22].
Smith
et
al.,
1997
showed
that
compared
to
a
control
group,
teachers
were
significantly
more
likely
to
report
having
6
voice
symptoms,
among
which
hoarseness
was
the
most
frequent,
and
5
related
physical
discomfort
symptoms
(tiring,
effortful,
ache,
uncomfortable
and
rough)
[23,24].
It
is
worth
mentioning
that
there
are
a
few
additional
studies
that
have
shown
a
different
impact
of
a
few
other
diseases
on
teachers:
an
excessive
rate
of
some
major
cancers,
in
particular
breast
[25]
and
thyroid
[26]
cancers
and
surprisingly
enough,
an
association
between
school
teaching
and
mortality
from
autoimmune
diseases
[27].
A
study
by
Kovess-Masféty,
said
that
teachers
do
not
seem
to
have
poorer
mental
health.
However,
their
physical
condition
is
characterized
by
a
higher
prevalence
of
health
problems
related
to
the
ENT
tract,
and
to
a
lesser
extent,
depending
on
the
gender,
to
skin,
eyes,
legs
and
lower
urinary
tract
[28].
Teachers
have
an
important
responsibility
in
tobacco
control
given
that
they
are
highly
respected
in
their
communities
as
they
influence
the
evolution
for
each
aspect
of
life
[29].
In
addition,
teachers
have
daily
interaction
with
students
and
thus
represent
an
influential
group
in
tobacco
smoking
control.
However,
this
potential
can
be
limited
if
teachers
use
tobacco
especially
in
the
presence
of
students
in
school
premises
[30].
Psychological
Teaching,
like
many
jobs,
is
potentially
stressful.
Some
sources
of
pressure
are
specific
to
teaching
but
others
are
common
to
various
professions
and
management
structures.
Pressures
which
teachers
have
encountered
include:
the
need
to
be
continually
vigilant
when
supervising
pupils,
verbal
abuse
from
pupils
and
parents,
parental
expectations,
the
requirement
to
manage
staff
including
support
assistants
and
other
teachers,
the
responsibility
for
head
teachers
to
effectively
manage
a
'business',
pressure
from
peers
and
colleagues,
coping
with
change
e.g.
in
management
systems,
examination
formats
and
the
curriculum
and
poor
or
inappropriate
management
including
delays
in
addressing
disciplinary
and
grievance
issues
[14].
Factors
Affecting
Teachers'
Mental
Health
These
include
the
lack
of
professional
aptitude
and
spirit,
occupational
hazards,
lack
of
social
prestige,
poor
salaries,
high
moral
expectations,
workload,
relationship
among
teachers,
relationship
between
the
administrator
and
teachers,
insecurity
of
service
and
lack
of
facilities
[14].
Study
design
Cross
sectional
research
design
Population
and
sampling
Male
teachers
in
Abha
City
constitute
the
study
population.
The
minimum
sample
size
for
this
study
has
been
decided
according
to
Swanson
and
Cohen
[31].
Following
a
simple
random
sample,
the
researcher
selected
an
equal
sample
from
primary,
intermediate
and
secondary
school
male
teachers
in
Abha
City.
All
respondent
teachers
were
exposed
to
the
questionnaire.
According
to
the
Ministry
of
Education
in
Aseer
region
data,
the
number
of
schools
in
Abha
city
are
96
schools
divided
into
46
primary,
33
intermediate
and
17
secondary
with
2219
teachers
in
all
levels.
So
the
average
number
in
each
school
is
about
23
teachers.
Number
of
teachers
in
primary
schools
was
1063,
intermediate
schools
was
763
and
secondary
schools
was
393
teachers.
Proportionate
sample
was
taken
from
each
level
according
to
the
following
formulas:
Primary=
384
(Sample
Size)
X
1063/
2219=184;
Intermediate=
384
(Sample
Size)
X
763/
2219
=132;
Secondary
=
384
(Sample
Size)
X
393/
2219=
68
So
in
Primary
level
we
selected
184
teachers
from
8
male
Schools
[due
to
socio-cultural
aspect]
randomly
from
the
total
primary
schools
to
cover
their
sample
size
and
avoided
non
responders
and
6
intermediate
schools
and
3
secondary
schools.
We
asked
all
school
teachers
to
participate
in
the
research.
If
extra
numbers
will
be
needed,
extra
schools
will
be
selected
randomly
soon.
Data
Collecting
Tool
Sample
of
Employment
Health
Questionnaire
(Department
of
Health)
[32].
Data
Design
A
self-administered
questionnaire
including
Personal
characteristics
as
Demographic
data,
medical
history
and
co-morbidities
and
Special
Habits,
was
designed.
Administrative
consideration:
The
Researcher
fulfilled
all
the
required
official
approvals.
The
researcher
explained
to
all
participants
how
to
fill
out
the
questionnaire
in
the
correct
way
and
how
to
answer
questions.
Ethical
consideration:
Before
Interviewing,
Informed
Consent
was
asked
from
all
samples
then
all
participants
had
the
right
not
to
participate
in
the
study
or
to
withdraw
from
the
study
prior
to
completion.
The
researcher
explained
the
purpose
to
all
respondents.
This
pre
measurement
education
is
an
important
part.
Confidentiality
and
privacy
were
guaranteed
for
all
participants.
Budget
This
study
was
carried
out
at
the
full
expense
of
the
researchers.
Statistical
Analysis
The
statistical
analysis
of
data
was
done
by
using
Excel
program
for
figures
and
SPSS
(SPSS,
Inc,
Chicago,
IL)
program
statistical
package
for
social
science
version
17
[33].
The
description
of
the
data
was
done
in
form
of
mean
(+/-)
SD
for
quantitative
data
and
Frequency
and
proportion
for
Qualitative
data.
The
analysis
of
the
data
was
done
to
test
statistical
significant
difference
between
the
groups.
For
quantitative
date,
student
t-test
was
used
to
compare
between
two
groups.
Chi
square
test
was
used
for
qualitative
data
and
odds
ratio
for
risk
assessment.
Pearson
Correlation
was
done
to
detect
association
between
variables.
P
is
significant
if
<
0.05
at
confidence
interval
95%.
In
socio-demographic
data
of
male
teachers
in
Abha
City
(N=384)
we
found
the
mean
age
of
39.31,
Gender
(male)
384
(100%),
experience
less
than
or
equal
to
10
years
was
109
(28.4%),
experience
more
than
or
equal
to
10
years
was
275
(71.6%)
and
level
of
schools:
primary
(47.9
%),
intermediate
(34.4
%)
and
secondary
(17.7%)
.
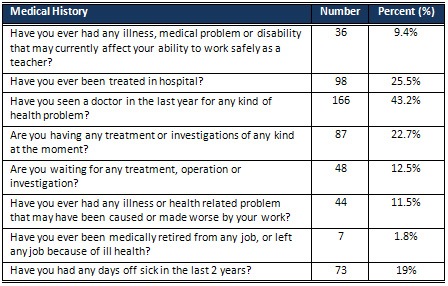
Table
1:
Medical
history
of
male
teachers
in
Abha
City
2014
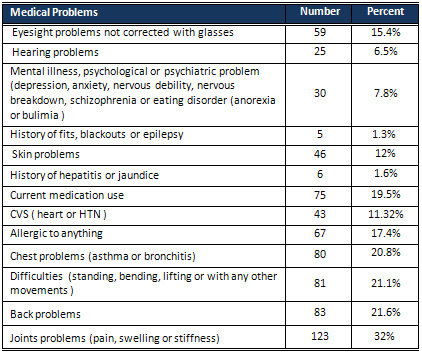
Table
2:
Medical
Problems
of
male
teachers
in
Abha
City
2014
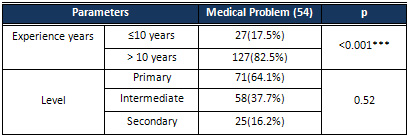
Table
3:
Relation
between
medical
problem
and
experience
years
and
level
of
male
teachers
This
study
was
done
to
assess
the
health
aspect
of
male
teachers
(384)
and
to
assess
level
of
job
satisfaction
of
male
teachers
in
different
grades
in
Abha
city.
A
simple
random
sample,
the
sample
from
primary,
intermediate
and
secondary
school's
male
teachers
in
Abha
City,
was
selected.
All
respondent
teachers
were
exposed
to
the
validated
questionnaire
to
assess
health
problem
[medical
history
and
co-morbidities]
and
work
place
risk
factors.
In
our
study
background
data
is
shown
as
age
39.31±7.96
[23:75]
years,
the
average
experience
years
were
16.1±7.43
[1:36]
years
and
71.6%
have
experience
more
than
10
years,
100
%
of
the
sample
was
males
due
to
socio-cultural
matters.
As
regards
the
educational
level
47.9%
were
from
primary
schools,
34.4%
from
intermediate
schools
and
17.7%
from
secondary
schools.
The
answers
about
some
medical
history
like
history
of
having
medical
problem
that
affects
teacher'
ability
(9.4%),
history
of
treating
in
hospital
(25.5%)
,
sick
leave
19%
are
all
within
the
accepted
range
but
seeing
a
doctor
in
last
year
(43.2%)
seems
to
be
higher
than
normal
range
and
mostly
due
to
respiratory
infections.
Kovess-Masféty,
V.,
et
al
2009
[28]
reported
in
France
that
among
teachers
their
physical
condition
is
characterized
by
a
higher
prevalence
of
health
problems.
Some
complaints
or
health
problems
among
teachers
in
our
study
regarding
eyesight
problems
recorded
(15.4%).
This
is
lower
than
Chong,
E.
Y.,
&
Chan,
A.
H.
(2010)
in
Hong
Kong
who
reported
32%
to
43%
eye
problems
among
teachers
[21].
Hearing
problems
in
6.5%;
this
is
lower
than
Martins,
R.
H.
G.
Et
al.,
2007
who
reported
25%
compared
to
10%
in
controls
with
an
acoustic
notch
predominating
(11.25%;
p<0.05),
due
to
excessive
classroom
noise
(93.5%)
and
auditory
symptoms
(65%).
Noise
levels
close
to
87dBA
were
recorded
in
classes
at
all
teaching
levels
[34].
Mental
illness,
psychological
or
psychiatric
problem,
including
depression,
anxiety,
nervous
debility,
nervous
breakdown,
schizophrenia
or
eating
disorder
was
7.8%
and
is
much
lower
than
Chong,
E.
Y.,
&
Chan,
A.
H.
(2010)
in
Hong
Kong
who
reported
high
prevalence
of
Pseudo-neurological
and
mental
disorders
among
teachers.
The
lower
rates
in
this
study
may
be
due
to
fear
of
social
stigma
in
our
society
and
under-estimation
and
ignorance
about
the
nature
of
psychological
diseases
[21].
The
skin
problems
(12%)
may
be
due
to
exposure
to
various
irritants,
either
chemical
or
biological
factors
in
schools.
This
is
lower
than
Chong,
E.
Y.,
&
Chan,
A.
H.
(2010)
who
reported
skin
problems
among
teachers
in
Hong
Kong
at
24.4%
[21].
The
history
of
hepatitis
or
jaundice
1.6%
is
much
less
than
prevalence
of
all
types
of
hepatitis
especially
in
the
southwestern
area
of
KSA
as
detected
by
Abdo,
A.
A.,
2012.
This
may
explained
by
health
appraisal
and
screening
being
done
before
job
allocation
[36].
The
heart
or
blood
pressure
problems
were
11.32%
and
this
rate
is
lower
than
community
prevalence
and
does
not
differ
than
the
level
in
developed
countries
as
detected
by
Ghabrah,
T.
M
et
al.,1998,
[16]
but
is
not
in
agreement
with
Ibrahim,
N.
K
et
al.,
2008
in
his
study
in
Jeddah
which
was
higher.
This
difference
may
come
from
the
detected
prevalence
of
risk
factors
like
obesity
which
was
lower
in
our
area
[17].
The
history
of
allergy
was
17.4%
due
to
exposure
to
different
chemical
and
biological
irritants
in
the
school
environment;
this
is
in
agreement
with
Chong,
E.
Y.,
&
Chan,
A.
H.
(2010).
A
study
in
Hong
Kong
reported
19%
prevalence
of
allergy
among
school
teachers
[21].
Suffering
from
asthma
or
chest
problem
was
reported
in
20.8%
due
to
drawbacks
from
allergy
or
recurrent
chest
infections.
This
is
higher
than
Chong,
E.
Y.,
&
Chan,
A.
H.
(2010)
[21]
in
Hong
Kong
who
reported
16.1%.
The
difference
could
be
explained
by
Al
Frayh,
A.
R.,
et
al.,
2001
[37]
who
reported
data
between
Riyadh
versus
Hail
(inland
desert
dry
environment)
and
Jeddah
versus
Gizan
(coastal
humid
environment)
which
revealed
that
the
prevalence
of
asthma
in
the
similar
populations
increased
significantly
from
8%
in
1986
to
23%
in
1995
due
to
environmental
changes.
History
of
Musculoskeletal
disorder
21.1%,
Low
back
pain
21.6%
and
joint
pain
32%.
These
high
rates
due
to
age,
length
of
employment
and
awkward
posture,
prolonged
posture,
static
works
and
repetition
are
the
cause
of
repetitive
strain
injuries
which
are
associated
with
higher
MSD
prevalence
rates
among
teachers.
This
is
matched
with
Erick
PN,
Smith
DR,2011
who
reported
that
the
schoolteachers
represent
an
occupational
group
among
which
there
appears
to
be
a
high
prevalence
of
MSD
[19].
In
our
study,
regarding
the
relation
between
medical
problem
and
experience
years
and
level
among
the
studied
Group
there
is
a
significant
association
between
medical
problem
and
experience
years
more
than
10
years
due
to
accumulation
of
stressors
and
chronic
diseases
so
the
effect
may
be
a
false
association
due
to
confounder
effect
of
the
aging
process.
There
was
no
significant
association
with
specific
educational
level;
this
may
explained
by
the
same
stressors
present
in
all
levels.
The
medical
problems
of
male
teachers
increase
with
age
increase.
The
health
status
of
male
teachers
is
not
optimal
since
a
high
percentage
of
them
have
to
see
a
doctor
each
year
and
one
third
of
them
are
currently
sick.
Moreover,
musculoskeletal
problems
are
quite
common
among
male
teachers.
Provision
of
health
educational
program
about
the
risks
which
the
teachers
have
been
exposed
to,
either
communicable
or
non-communicable.
Establishment
of
a
specific
health
program
for
teachers
caring
with
their
health
status.
More
availability
of
preventive
health
care
measures
to
avoid
co-
morbidities
associated
with
work
environment.
Multidisciplinary
team
approach
toward
the
screening
and
diagnosis
of
health
hazards
among
teachers
that
consists
of
"Clinical,
Laboratory,
radiological,
Occupational
and
epidemiological
researcher
teams".
1.
Smylie
MA.
Teacher
stress
in
a
time
of
reform.
In
R.
Vandenberghe
&
AM.
Huberman
(Eds.),
Understanding
and
preventing
teacher
burnout
(pp.
59-84).
Cambridge:
Cambridge
University
Press,
1999.
2.
Ewing
RA,
Smith
DL.
Retaining
quality
beginning
teachers
in
the
profession.
English
Teaching:
Practice
and
Critique,
2003;
2(1):
15-32.
3.
Ramsey
G.
Quality
matters.
Revitalising
teaching:
Critical
times,
critical
choices.
Sydney:
New
South
Wales
Department
of
Education
and
Training.
2000,
Retrieved
10
August
2004,
from
http://www.det.nsw.edu.au/teachrev/reports/
4.
Macdonald
D.
Teacher
attrition:
a
review
of
literature.
Teaching
and
Teacher
Education,
1999;
15:
835-848.
5.
Nelson
B.
Our
universities:
Backing
Australia's
future.
Certo,
J.L.,
&
Fox,
J.E.
(2002).
Retaining
quality
teachers.
The
High
School
Journal,
2003;
86(1):
57-
75.
6.
Dunn
D.
Teaching
about
the
good
life:
Culture
and
subjective
well-being.
Journal
of
Social
and
Clinical
Psychology,
2002;
21(2),
218-220.
7.
Brouwers
A,
Tomic
W.
A
longitudinal
study
of
teacher
burnout
and
perceived
self-
efficacy
in
classroom
management.
Teaching
and
Teacher
Education,
2000;
16:
239-253.
8.
Smith
M,
Bourke
S.
Teacher
stress:
Examining
a
model
based
on
context,
workload,
and
satisfaction.
Teaching
and
Teacher
Education,
1992;
8(1):
31-46.
9.
Singh
K,
Billingsley
BS.
Intent
to
stay
in
teaching.
Remedial
&
Special
Education,
1996;
17(1):
37-48.
10.
The
Management
of
Health
and
Safety
at
Work
Regulations
1999.
11.
Desjean-Perrotta
B.
Developing
a
fitness
to
teach
policy
to
address
retention
issues
in
teacher
education.
Childhood
Education,
2006;
83(1):
23-28.
12.
Alzaidi
AM.
A
Qualitative
Study
of
Job
Satisfaction
among
Secondary
School
Head
Teachers
in
the
City
of
Jeddah,
Saudi
Arabia.
ARECLS,
2008;
4:
1-15.
13.
Chance
P.
That
burned
out,
used-up
feeling
Psychology
Today.
Prentice
Hall,
New
Delhi.1981.
14.
Seibt,
R,
Lützkendorf
L,
Thinschmidt
M.
Risk
factors
and
resources
of
work
ability
in
teachers
and
office
workers.
In
International
Congress
Series.
Elsevier,
2005;
1280:
310-315.
15.
Helmert
U,
Shea
S,
Bammann
K.
The
impact
of
occupation
on
self-reported
cardiovascular
morbidity
in
western
Germany:
gender
differences.
Reviews
on
environmental
health,
1997;
12(1):
25-42.
16.
Ghabrah
T
M.,
Bahnassy,
A
A.,
Abalkhail
B
A,
Soliman
NK.,
Milaat,
WA.
The
prevalence
of
cardiovascular
risk
factors
among
school
teachers
in
Jeddah,
Saudi
Arabia.
Journal
of
the
Saudi
Heart
Association,
1998;
10(3):
189-195.
17.
Ibrahim
NK,
Hijazi
NA,
Al-Bar
AA.
Prevalence
and
determinants
of
prehypertension
and
hypertension
among
preparatory
and
secondary
school
teachers
in
Jeddah.
J
Egypt
Public
Health
Assoc,
2008;
83(3-4):183-203.
18.
Deyanov
C,
Hadjiolova
I,
Mincheva
L.
Prevalence
of
arterial
hypertension
among
school
teachers
in
Sofia.
Reviews
on
environmental
health,
1994;
10(1):
47-50.
19.
Erick
PN,
Smith
DR.
A
systematic
review
of
musculoskeletal
disorders
among
school
teachers.
BMC
musculoskeletal
disorders,
2011;
12(1):
260.
20.
Maguire
M,
O'Connell
T.
Ill-health
retirement
of
schoolteachers
in
the
Republic
of
Ireland.
Occupational
Medicine,
2007;
57(3):
191-193.
21.
Chong
EY,
Chan
AH.
Subjective
health
complaints
of
teachers
from
primary
and
secondary
schools
in
Hong
Kong.
International
journal
of
occupational
safety
and
ergonomics,
2010;
16(1):
23-39.
22.
Chaiklieng
S,
Suggaravetsiri
P.
Risk
factors
for
repetitive
strain
injuries
among
school
teachers
in
Thailand.
Work:
A
Journal
of
Prevention,
Assessment
and
Rehabilitation,
2012;
41:
2510-2515.
23.
Titze
IR,
Lemke
J,
Montequin
D.
Populations
in
the
US
workforce
who
rely
on
voice
as
a
primary
tool
of
trade:
a
preliminary
report.
Journal
of
Voice,
1997;
11(3):
254-259.
24.
Williams
NR.
Occupational
groups
at
risk
of
voice
disorders:
a
review
of
the
literature.
Occupational
medicine,
2003;
53(7):
456-460.
25.
Bernstein
L,
Allen
M,
Anton-Culver
H,
Deapen
D,
Horn-Ross
PL,
Peel
D
et
al.
High
breast
cancer
incidence
rates
among
California
teachers:
results
from
the
California
Teachers
Study
(United
States).Cancer
Causes
&
Control,
2002;
13(7):
625-635.
26.
Lope
V,
Pollán
M,
Gustavsson
P,
Plato
N,
Pérez-Gómez
B,
Aragonés
N,
López-Abente
G.
Occupation
and
thyroid
cancer
risk
in
Sweden.
Journal
of
occupational
and
environmental
medicine,
2005;
47(9):
948-957.
27.
Walsh
SJ,
DeChello
LM.
Excess
autoimmune
disease
mortality
among
school
teachers.
The
Journal
of
rheumatology,2001;
28(7):
1537-1545.
28.
Kovess-Masféty
V,
Sevilla-Dedieu
C,
Rios-Seidel
C,
Nerrière
E,
Chee
CC.
Do
teachers
have
more
health
problems?
Results
from
a
French
cross-sectional
survey.
BMC
Public
Health,
2006;
6(1):
101.
29.
Al-Naggar
RA,
Jawad
AA,
&Bobryshev
YV.
Prevalence
of
cigarette
smoking
and
associated
factors
among
secondary
school
teachers
in
Malaysia.
Asian
Pacific
J
Cancer
Prev,
2012;
13:
5539-5543.
30.
GTSS
Collaborative
Group.
The
Global
School
Personnel
Survey:
a
cross?country
overview.
Tobacco
Control,
2006;
15(Suppl
2),
ii20.
31.
Swanson
Cohen
JM.
Color
vision.
Ophthalmol
Clin
North
Am.
2003;
16(2):179-203.
32.
Department
of
Health,
Department
for
Education
and
Employment,
Public
Health
Laboratory
Service
1999
.
33.
SPSS
Inc..
Statistical
Package
for
the
Social
Sciences,
17.
Chicago,
Illinois:
SPSS
Inc.
2008.
34.
MartinsRHG,
Tavares
ELM,
Lima
Neto
AC,
Fioravanti
MP.
Occupational
hearing
loss
in
teachers:
a
probable
diagnosis.
Revista
Brasileira
de
Otorrinolaringologia,
2007;
73(2):
239-244.
35.
Al
Rajeh
S,
Awada
A.
Stroke
in
Saudi
Arabia.
Cerebrovascular
Diseases,
2002;
13(1):
3-8.
36.
Abdo
AA,
Sanai
FM,
Al-Faleh
FZ.
Epidemiology
of
viral
hepatitis
in
Saudi
Arabia:
Are
we
off
the
hook?.
Saudi
journal
of
gastroenterology:
official
journal
of
the
Saudi
Gastroenterology
Association,2012;
18(6):
349.
37.
Al
Frayh
AR,
Shakoor
Z,
ElRab
MO,
Hasnain
SM.
Increased
prevalence
of
asthma
in
Saudi
Arabia.
Annals
of
Allergy,
Asthma
&
Immunology,
2001;
86(3):
292-296.
|
|
.................................................................................................................

|
| |
|
