|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
|
|
|
|
........................................................
|
Original
Contribution/Clinical Investigation
|
|
|
<-- Abu Dhabi -->
Knowledge,
attitude and behaviour of asthmatic patients
regarding asthma in primary care setting in
Abu Dhabi, United Arab Emirates
[pdf version]
Osama Moheb Ibrahim Mohamed, Wael Karameh Karameh
<-- Egypt -->
DASH Diet: How
Much Time Does It Take to Reduce Blood Pressure
in Pre-hypertensive and Hypertensive Group 1
Egyptian patients?
[pdf version]
Rehab Abdelhai, Ghada Khafagy, Heba Helmy
<-- Egypt -->
Assessment of TB
stigma among patients attending chest hospital
in Suez Canal University area, Egypt
[pdf version]
Nahed Amen Eldahshan, Rehab Ali Mohammed, Rasha
Farouk Abdellah, Eman Riad Hamed
<-- Egypt -->
Awareness
of diabetic retinopathy in Egyptian diabetic
patients attending Kasra Al-Ainy outpatient
clinic: A cross-sectional study
[pdf version]
Marwa Mostafa Ahmed, Mayssa Ibrahim Ali, Hala
Mohamed El-Mofty, Yara Magdy Taha
<-- Iraq -->
Estimation of
some biophysical parameters in semen of fertile
and infertile patients
[pdf version]
Dhahir Tahir Ahmad, Suhel Mawlood Alnajar, Tara
Nooradden Abdulla, Zhyan Baker Hasan
|
|
........................................................ |
Medicine and Society
|
|
<-- Iraq -->
Celebrating lives
from the Region
[pdf version]
Lesley Pocock
<-- Regional/International -->
Health
Promotion, Disease Prevention and Periodic Health
Checks: Perceptions and Practice among Family
Physicians in Eastern Mediterranean Region
[pdf version]
Waris Qidwai, Kashmira Nanji, Tawfik A M Khoja,
Salman Rawaf, Nabil Yasin Al Kurashi, Faisal
Alnasir, Mohammed Ali Al Shafaee, Mariam Al
Shetti,Nagwa Eid Sobhy Saad, Sanaa Alkaisi,
Wafa Halasa, Huda Al-Duwaisan, Amal Al-Ali
<--
Australia/Iran -->
Virology
vigilance - an update on MERS and viral mutation
and epidemiology for family doctors
[pdf version]
Lesley Pocock, Mohsen
Rezaeian
|
........................................................
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| July / August
2015 - Volume 13 Issue 5 |
|
Knowledge,
attitude and behaviour of asthmatic patients regarding
asthma in primary care setting in Abu Dhabi, United
Arab Emirates
Osama
Moheb Ibrahim Mohamed
(1)
Wael Karameh Karameh (2)
(1) Osama Moheb Ibrahim Mohamed, MBBCh, MSc,
MD
Consultant Family Medicine, Ambulatory Health
Services, SEHA corporate, Abu Dhabi, UAE
(2) Wael Karameh Karameh, MD, ABFM,
Consultant Family Medicine, Ambulatory Health
Services, SEHA corporate, Abu Dhabi, UAE
Correspondence:
Dr. Osama Moheb Ibrahim Mohamed
Email: osamamohebibrahim@gmail.com
|
Abstract
Background: Adequate
knowledge, positive attitude and behaviour
as well as proper inhaler use of asthmatic
patients are prerequisites for optimal
management of bronchial asthma.
Objectives: To
assess the knowledge, attitude and practice
of patients with asthma with respect to
their disease and to examine their skills
in using inhaled medications.
Patients and methods: In
a cross sectional analytic study, a sample
of 100 asthmatic patients was selected
from patients attending Al Bateen Family
Medicine clinic in Abu Dhabi during the
period from August 2011 to July 2012.
Inclusion Criteria were adult patients
known asthmatic for one year or more;
patients using inhalers or Diskus inhaler
Informed consent was obtained from every
patient who agreed to enrol in the study.
Each patient responded to a structured
questionnaire assessing his/her knowledge
about asthma aetiology, pathophysiology,
symptoms, treatment and triggering factors;
and evaluating his/her attitude and behaviour
regarding asthma diagnosis, inhalers,
anti-inflammatory drugs and non-medical
methods of treatment , and assessment
of their inhaler skills.
Results: There
were 52% males and 48% females enrolled
in the study. The main sources of information
about asthma were health workers (56%)
and Newspapers and magazines (18%). 70%
believed that asthma can be life threatening;
asthma was believed to be initiated by
infections in 86% of patients and weather
changes by 49%. The reasons for acute
exacerbations were perfumes (87%) and
upper respiratory tract infection (86%).
About 59% of the patients did not use
inhaled preventers regularly when prescribed
because they believe that inhaled therapy
is habit forming; (34%) felt uncomfortable
taking asthma medication at work or public
places or away from home, and 42% of patients
avoided exercise due to fear of acute
exacerbations. There were (71%) using
MDI, (28%) using Diskus inhaler and (13%)
using turbo haler. Only a few patients
had the correct skills using Metered-Dose
Inhaler ( MDI), Discus or turbo haler;
the mean score of correct use of MDI was
5+.47 out of 8; the mean score of correct
use of discus was 4+.82 out of 7; the
mean score of correct use of turbo haler
was 3+ 0.67 out of 6. Most patients did
not use peak flow meter (PFM) in asthma
management. About 5% of asthmatic patients
tried non-medical methods for the purpose
of cure. These included traditional healers.
Conclusion: Asthmatic
patients in Bateen Clinic have false beliefs
and poor inhaler skills about asthma management.
Most of them use inhalers for treatment
of asthma attacks and less than half do
not use preventers regularly when prescribed.
Most patients believe that preventer therapy
lead to its addiction; most of them are
lacking inhaler skills especially coordination
actuation with inhalation; most patients
avoid exercise to avoid acute exacerbations.
Patients' ideas, concerns and fears regarding
asthma management should be explored during
consultation; inhaler skills should be
reviewed also in each visit.
Key words: asthma,
primary care, Abu Dhabi
|
Asthma is a chronic inflammatory disorder of
the airways. Anti-inflammatory agents such as
inhaled steroids, leukotriene antagonists. are
the mainstay of its management. Under-utilization
of these agents and reliance on reliever medication
has been reported in much of the literature.
(1-2)
Bronchial asthma is one of the most common chronic
respiratory disorders among all age groups with
a reported prevalence of 5 to 10%. (3) During
the last decades studies from different countries
keeping appropriate statistics have reported
a significant rise in asthma morbidity and mortality.
(3)
The prevalence of physician diagnosed asthma
among governmental primary school children in
the United Arab Emirates was 13%, in addition
the wheeze by history was 15.6%. (4). Another
study carried out by Al Ain University estimated
13 % prevalence of asthma among local Emirates
patients. (5)
Adherence to prescribed inhaled corticosteroids
is notoriously poor. Even in observational studies
where patients were aware of being monitored,
average adherence was only 63% to 65 %.(5) Non-adherence
to long-term inhaled corticosteroids is thought
to be a major reason for treatment failure.
(6)
It is known that adherence to the use of inhalers
is generally poor. Studies have shown that on
average, only 63-65% of participants adhere
to their inhaled corticosteroids even while
under the period of observation. It is likely
that adherence over the longer term is much
less and this is suspected to be a major reason
for treatment of asthma to fail (7).
Providing information only, versus providing
information plus teaching actual skills as part
of asthma education intervention trials has
not been shown to change patients' self-management
behaviours. A scientific review of 12 randomized
controlled trials showed that providing information
only increased subjects' knowledge of asthma
but did not reduce hospitalizations, emergency
room visits, unscheduled doctor visits or lost
work days and it did not lead to improved lung
function or adherence to medication (8).
Asthmatics have been classified into two groups:
Deniers reject the fact that they have a chronic
illness or are "asthmatic". This group
of people tends not to take prophylactic medication.
They may fear dependency and lack of perceived
control over their illness but as a consequence
end up "over-using" B-adrenoceptor
agonists. Acceptors understand the chronic nature
of asthma and are more likely to adhere to prophylaxis
and resort to using short-acting B-adrenoceptor
agonists only when needed in an acute attack
(9).
Many asthmatic patients think of asthma as being
an intermittent illness that does not warrant
daily treatment - "it's only asthma",
(10) while others believe treatment is only
necessary when there is an exacerbation of their
disease (11). Adolescents may think they have
"grown out" of a childhood illness
(10). Teenagers may also be reluctant to ask
others to stop smoking in their presence and
may even smoke themselves partly due to wanting
to 'fit-in' with their peers (12). Many patients,
especially children, may be embarrassed to use
their inhalers in front of others and do not
want the stigma associated with a disease (12).
On the other hand, adherence can be increased
in patients who have been hospitalized for their
asthma as they realize the seriousness of their
disease (12).
Misperceptions about the role of inhaled corticosteroids
(ICS) in asthma are common and can contribute
to lack of adherence in use. Many patients are
concerned about the safety of the medication
and do not understand why ICS are necessary
and these factors are believed to be key contributors
to lack of adherence (15). Due to the fact that
corticosteroids may not relieve symptoms during
an acute attack, some patients may think the
medication is ineffective and therefore not
necessary (16). 'Steroid phobia' is common,
occurring in up to 46% of people who have been
prescribed ICS (16). Studies have shown that
only 45% of ICS prescribed are actually taken
(13, 14).
Barriers to asthma medication adherence are
: concern about drug cost and safety; belief
that the asthma is not severe enough to warrant
daily treatment; concern about drug dependence
or diminished effectiveness over time; peer
stigmatization; forgetfulness; belief that asthma
medication is ineffective; denial that one is
asthmatic; difficulty using asthma inhalers;
inconvenience; fear of medication side-effects;
embarrassment and laziness (17).
In this study we tried to figure out our patients'
knowledge, attitude, skills and barriers regarding
asthma management to improve their care.
This
was
a
descriptive,
cross
sectional
study.
It
had
been
carried
out
in
a
Family
Medicine
Clinic,
which
is
a
part
of
Ambulatory
Health
Services,
SEHA
corporate,
Abu
Dhabi,
UAE.
One
hundred
asthmatic
patients
were
selected
from
those
presenting
to
a
Family
Medicine
clinic.
Inclusion
criteria
were
age
18
years
and
above,
known
asthmatic
for
one
year
or
more.
Exclusion
criteria
were
age
less
than
18
years
and
patients
with
COPD.
Patients
responded
to
a
structured
questionnaire
assessing
their
Demographic
data
(age,
sex,
education,
employment
status,
duration
of
asthma),
knowledge
about
asthma
aetiology,
symptoms,
triggering
factors,
pathophysiology
and
management,
and
requiring
information
about
their
attitude
and
behaviour
towards
the
diagnosis
of
asthma,
and
use
of
inhalers.
Patients
were
asked
to
demonstrate
the
use
of
their
inhaler
and
the
investigator
observed
the
different
steps.
All
patients
gave
their
informed
consent
before
participating
in
the
study.
Data
obtained
was
analysed
using
the
statistical
package
for
the
social
sciences
(SPSS)
version
14.
The
study
proposal
was
approved
by
the
Institute
Review
Board
at
Sheikh
Khalifa
Medical
City/managed
by
Cleveland
Clinic
under
the
reference
of
REC-14.07.2011(RS-168).
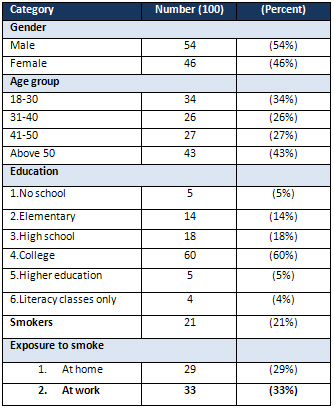
Patients'
characteristics:
A
total
of
100
asthmatic
patients
were
enrolled
in
the
study.
Males
were
52%
and
females
were
48%.
The
majority
of
patients
(43%)
were
above
50
years.
About
5%
were
without
education
and
60%
had
college
education.
(Table
1)
Table
1:
Demographic
data
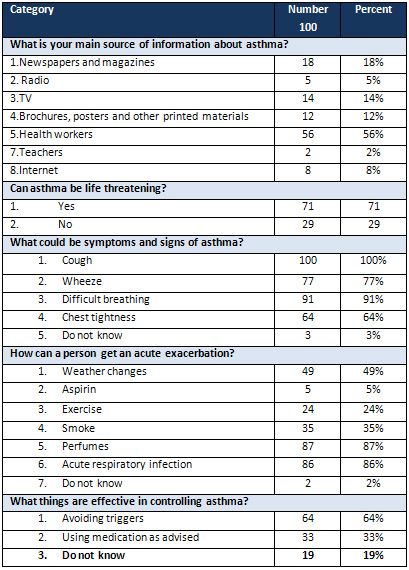
Patients'
knowledge:
Health
workers
were
the
main
source
(56%)
of
patients'
information.
Asthma
was
believed
to
be
life
threatening
by
(71%)
of
patients.
The
main
causes
of
acute
exacerbations
were
acute
respiratory
infection
(86%)
and
perfumes
(87%);
most
patients
know
symptoms
of
acute
attacks.
(Table
2)
Table
2:
Patient
knowledge
about
asthma
aetiology,
pathophysiology
and
triggering
factors
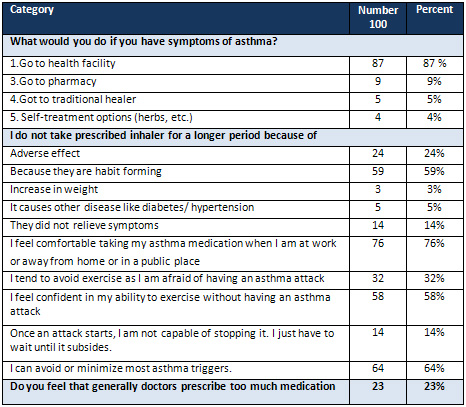
Patients'
attitude
and
behaviour:
Table
3
describes
the
attitude
of
patients
towards
asthma
and
their
behaviour
regarding
use
of
inhalers
and
preventive
therapy.
(57%)
of
patients
usually
seek
medical
care
for
treatment
of
asthma.
A
total
of
(59%)
of
asthmatic
patients
did
not
use
the
anti-inflammatory
drugs
(the
preventers)
in
the
form
of
steroid
inhalers
when
prescribed
because
they
were
afraid
of
lifelong
dependence
on
inhalers
.Most
patients
(76%)
have
felt
comfortable
taking
asthma
medication
when
they
were
at
work
or
away
from
home
or
in
a
public
place.
Table
3:
Attitude
and
behaviour
of
patients
towards
their
illness
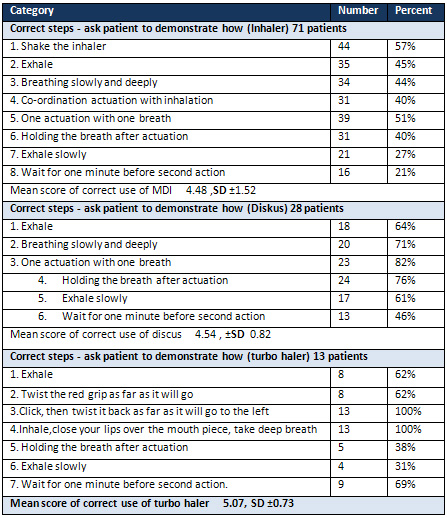
Technique
of
inhaler,
Diskus
and
turbo
haler
There
were
71
(71%)
of
patients
used
MDI,
18
(18%)
used
Diskus
inhaler
and
13
(13%)
used
Turbo
haler.
Patient
demonstrated
the
use
of
their
inhalers
correctly
as
follows:
MDI
(40.62%),
Diskus
(66.66%)
and
Turbo
haler(66%)
respectively
.
The
observed
different
steps
in
using
inhaler
techniques
are
shown
in
Table
4.
Table
4:
Technique
of
inhaler,
discus
and
turbo
haler
use
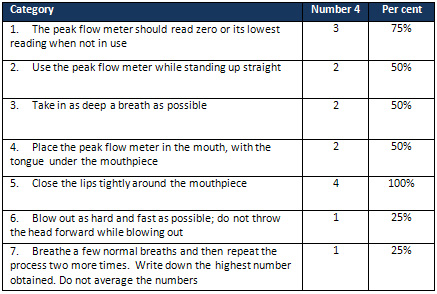
Only
4
(4%)
of
study
population
used
PFM
for
Follow
up
of
asthma
management.
Only
1
patient
knew
fully
how
to
use
PFM
in
a
correct
way.
(Table
5).
Table
5:
Technique
of
peak
flow
meter
use
Successful
asthma
management
depends
on
many
factors;
these
include
sufficient
knowledge
and
positive
attitude.
A
patient
with
asthma
should
understand
the
basic
pathophysiology
of
asthma,
know
symptoms
of
acute
attacks,
identify
triggering
factors
and
be
able
to
take
appropriate
steps
to
manage
their
illness.
On
the
other
hand,
an
asthmatic
patient
should
have
a
positive
attitude
towards
asthma
including
willingness
to
follow
the
physician's
instructions
to
manage
the
disorder.
These
two
factors
interact
with
each
other
and
with
other
important
factors
such
as
inhaler
technique
skills
to
determine
the
overall
patient's
compliance.
To
control
these
factors,
it
is
important
to
determine
the
level
of
patients'
knowledge,
to
evaluate
their
attitudes
regarding
asthma
and
to
assess
the
patients'
skills
in
using
medications
in
order
to
plan
interventional
programmes
that
may
direct
their
behaviour
towards
proper
management
of
their
illness,
thus
reducing
the
overall
morbidity
and
mortality.
In
this
study,
knowledge,
attitude,
skills
and
behaviour
of
asthmatic
patients
regarding
asthma
were
assessed
using
a
questionnaire.
(19)
The
patients
attended
a
family
Medicine
Clinic
in
Abu
Dhabi
City.
Most
of
them
(65%)
were
educated
to
a
college
or
higher.
The
reliability
of
the
questionnaire
used
in
assessment
was
revised
by
members
of
the
Research
Committee
in
Al
Bateen
Family
health
Center
and
in
Sheikh
Khalifa
Medical
City
managed
by
Cleveland
Clinic.
In
this
study
the
main
source
of
patients'
information
regarding
asthma
was
the
health
worker
(56%).
This
result
is
consistent
with
the
results
of
a
study
conducted
to
assess
patients'
knowledge
in
a
tertiary
care
hospital.
The
study
found
that
(85%)
of
patients
reported
that
doctors
were
the
main
source
of
information.
This
study
suggests
that
patients
look
up
to
health
care
providers
as
an
important
source
of
information
therefore
clinicians
should
continue
to
play
an
important
role
in
disseminating
information
on
asthma.(20)
In
this
study
(59%)
of
patients
do
not
take
their
prescribed
inhaler
for
a
longer
period
because
they
believe
that
these
medications
are
habit
forming.
This
is
again
consistent
with
the
attitude
of
asthmatics
in
other
studies;
it
is
reported
that
50%
of
patients
suffering
from
chronic
diseases
do
not
comply
with
the
doctor's
advice
on
treatment
(21)
though
there
has
been
little
agreement
about
the
causes
of
noncompliance.
Among
asthmatics
there
are
deniers
and
acceptors
of
the
diagnosis,
including
misconceptions
about
inhalers
(24),
and
it
is
postulated
that
these
beliefs
and
attitudes
influence
the
medication
practice.
(22)
Another
factor
that
affects
patients'
compliance
to
treatment
is
the
side
effects
of
medications.
(24%)
of
asthmatic
patients
in
this
study
were
reluctant
to
use
preventive
inhaler
regularly
because
of
fear
of
side
effects
that
affected
their
compliance
to
treatment
and
their
use
of
inhalers.
Many
of
these
patients
gave
explanations
like
inhalers
make
their
symptoms
continue
for
a
longer
time
and
they
may
become
dependent
on
inhalers
for
the
rest
of
their
lives
if
they
started
using
them.
However,
the
clear
explanation
for
this
wrong
behaviour
is
most
probably
that
the
use
of
inhalers
makes
relatives
and
colleagues
know
that
they
suffer
from
asthma,
which
is
regarded
as
a
stigma.
That
is
why
they
are
reluctant
to
accept
using
them.
Patients
often
combine
biomedical
facts
with
alternative
beliefs
and
practices
in
their
approach
to
illness
and
physicians
should
be
aware
of
this
in
order
to
optimize
health
education
and
clinical
management.
(24)
In
this
study
only
4%
of
patients
were
using
a
Peak
flow
meter
for
monitoring
their
asthma.
One
of
the
explanations
is
that
prescribing
peak
flow
meters
and
giving
self-management
guidelines
to
all
asthma
patients
is
unlikely
to
improve
mortality
or
morbidity.
Patients
whose
asthma
is
severe
may
benefit
from
such
an
intervention.
(25)
Asthmatic
patients
in
Bateen
Clinic
have
poor
inhaler
skills
and
false
beliefs
about
asthma
management.
Most
of
them
use
inhalers
for
treatment
of
asthma
attacks
and
less
than
half
do
not
use
preventers
regularly
when
prescribed.
Most
patients
believe
that
preventer
therapy
leads
to
its
addiction;
most
of
the
patients
are
lacking
inhaler
skills
especially
coordination
actuation
with
inhalation;
most
patients
avoid
exercise
to
avoid
acute
exacerbations.
Patients'
ideas,
concerns
and
fears
regarding
asthma
management
should
be
explored
during
consultation.
Inhaler
skills
should
be
reviewed
also
in
each
visit.
1.
Sin
DD,
Tu
JV.
Under
use
of
inhaled
steroids
therapy
in
elderly
patient
with
asthma.
Chest
2001;
119:
720-725.
2.
Terr
AL,
Bloch
DA.
Trends
in
asthma
therapy
in
United
States
1965
to
1992.Ann
Allergy
Asthma
Immunol
1996;
76:
273-281.
3.
Williams
MH.
Increasing
severity
of
asthma
from
1960-1987.
N
Engl
J
Med
1989;
320:
1015-16.
4.
Ministry
of
Health
UAE
2004.
http://213.42.151.126/en/Page_573.aspx
5.
European
Journal
of
Epidemiology
Volume
10,
Number
3,
271-278,
DOI:
10.1007/BF01719349.
Department
of
Internal
Medicine,
Faculty
of
Medicine
and
Health
Sciences,
POB
17666,
United
Arab
Emirates
University,
Al-Ain,
United
Arab
Emirates.
6.
Fact
sheet:
Asthma:
A
worldwide
problem.
Document
accessed
on
February
8,
2005
at
website
of
International
Union
Against
Tuberculosis
and
Lung
Diseases
(IUATLD)
www.iuatld.org
7.
Hilton
S,
Sibbald
B,
Anderson
HR,
et
al.
Controlled
evaluation
of
the
effects
of
patient
education
on
asthma
morbidity
in
general
practice.
Lancet
1986;
1:
26-29.
8.
Maiman
LA,
Green
LW,
Gibson
G,
et
al.
Education
for
self-treatment
by
adult
asthmatics.
JAMA
1979;
241:
1919-1922.
9.
Buston
KM,
Wood
SF.
Non-compliance
amongst
adolescents
with
asthma:
listening
to
what
they
tell
us
about
self-management.
Fam
Pract
2000;
17:
134-8.
10.
Chambers
CV,
Markson
L,
Diamond
JJ,
et
al.
Health
beliefs
and
compliance
with
inhaled
corticosteroids
by
asthmatic
patients
in
primary
care
practices.
Respir
Med
1999;
93:
88-94.
11.
Rubin
BK.
Adherence
to
asthma
therapy:
the
“Blocked
Receptor”.
Pediatr
Pulmonol
2004;
26
(Suppl.):
36-7.
12.
Pound
P,
Britten
N,
Morgan
M,
et
al.
Resisting
medicines:
A
synthesis
of
qualitative
studies
of
medicine
taking.
Soc
Sci
Med
2005;
61:
133-55.
13.
Dowell
J,
Hudson
H.
A
qualitative
study
of
medicine-taking
behaviour
in
primary
care.
Fam
Pract
1997;
14:
369-75.
14.
Garg
VK,
Bidani
R,
Rich
EP,
et
al.
Asthma
patients’
knowledge,
perception,
and
adherence
to
the
asthma
guidelines.
J
Asthma
2005;
42:
633-8.
15.
Rao
VU,
Apter
AJ.
Steroid
phobia
and
adherence:
problems,
solutions,
impact
on
benefit/risk
profile.
Immunol
Allergy
Clin
North
Am
2005;
25:
581-95.
16.
Horne
R,
Weinman
J.
Patients’
beliefs
about
prescribed
medicines
and
their
role
in
adherence
to
treatment
in
chronic
physical
illness.
J
Psychosom
Res
1999;
47
(6):
555-67.
17.
Bruce
Bender,
PhD,
and
colleagues
reported
at
the
2006
annual
meeting
of
the
American
Academy
of
Allergy,
Asthma
&
Immunology
(AAAAI).
18.
Diagnostic
and
Therapeutic
Guideline
of
Asthma
(2000),
and
Pocket
Guide
for
Asthma
Management
and
Prevention
in
Children:
A
Pocket
Guide
for
Physicians
and
Nurses
(2005)
19.
JK,
Stout
C,
Brandon
M,
et
al.
The
knowledge,
attitude
and
self
efficacy
Asthma
Questionnaire.
Chest
1993;104:1144-48.
20.
She
Ming
Chai,
King
Leong
Tan
,
Joslin
liling
Wong
and
Philip
Eng.
Asthma
knowledge
among
adults
asthmatic
outpatients
in
a
tertiary
care
hospital.
Asian
pacific
Journal
of
allergy
and
immunology
(2004)
22:81-89.
21.
Carr
A.
Editorial.
British
Journal
of
General
Practice;
1990,
40
(Sept),
358-
360.
22.
Stockwell
Morris
L,
Schulz
RM.
Patient
compliance-
an
overview.
Journal
of
Clinical
Pharmacy
and
Therapeutics
1992;
17:
283-295.
23.
Kriner
P,
Bernal
Y,
Binggeli
A,
Ornelas
I.
Attitudes,
beliefs,
and
practices
regarding
asthma
care
among
providers
and
adult
asthmatics
in
Imperial
Country.
Californian
Journal
of
Health
Promotion
2003;
1:88-100.
24-.Pachter
LM,
Weller
SC,
Baer
RD,
Garcia
JE,
Trotter
RT,
Glazer
M.
Variation
inAsthma
beliefs
and
practices
among
mainland
Puerto
Ricans,
Mexican-
Americans,
Mexicans
and
Guatemalans.
Journal
of
Asthma
2002;
39:119-
134.
25.
No
authors.
Effectiveness
of
routine
self-monitoring
of
peak
flow
in
patients
with
asthma.
Grampian
Asthma
Study
of
Integrated
Care
(GRASSIC),
BMJ.
1994
Feb
26;
308(6928):564-7.
|
|
.................................................................................................................

|
| |
|
