|
Indications and findings
of upper gastrointestinal endoscopy (UGIE) in
patients of Gizan, Saudi Arabia: A retrospective
study
Hussein Ageely
Correspondence:
Hussein Ageely
Department of Internal Medicine,
Faculty of Medicine,
Jazan University,
Jazan, Kingdom of Saudi Arabia
Email: hageely@me.com
|
Abstract
Objectives:
The objectives of this study were to identify
the common indications and findings of
upper gastrointestinal (GI) endoscopy
in patients presenting to King Fahd Central
Hospital (KFCH) in Gizan town Southwest
Saudi Arabia, and to furthermore, determine
the associations between them and the
common endoscopic findings and some selected
clinical and demographic variables.
Patients and Methods: This was
a retrospective study carried out at KFCH
over an 11 year period from 1994 to 2005.
All patients (3287), age of 12 years and
above referred for endoscopy unit were
enrolled in this study. Standardized form
(sheet) was used to collect all relevant
data including age, gender, and indications
for the procedure, clinical examination
and endoscopic findings.
Results: A total of 3287 patients
were included in the study with a mean
age of 45.3 years (SD ± 18.4);
males patients comprised 70.1%. Indications
for upper GI endoscopy included upper
gastrointestinal (GI) bleeding (23.3%),
with a significant difference between
males and females (p-value = 0.000), Epigastric
pain (15.7%), Acid Peptic Disease (APD)
(14.4%), Dyspepsia (7.5%) and regular
follow-up (6.5%). Among patients who underwent
UGI E, (21.3%) had normal endoscopic findings.
Three common findings were; Oesoph Varices
(15.2%), Gastritis (14.0%) and Oesophagitis
(10%). Gender and age of patient were
associated with a significantly high risk
of Oesoph. Varices (OR=3.43 and 1.95 respectively;
p-value< 0.001 for all).
Conclusion: The results of the
study suggested that UGI bleeding was
the main indication for UGI E in the vast
majority of our patients. In addition
to that three common diseases; Oesophageal
Varices, Gastritis and Oesophagitis were
the main findings of the UGI E among the
study population. Preventive measures
should be adopted to cope with the situation
and to prevent complications of esophageal
and gastritis diseases among the Gizan
population.
Key words:
Dyspepsia, indications, Gizan, Oesophageal
Varices, Gastritis, Oesophagitis
|
Upper gastrointestinal endoscopy (UGIE), or
oesophagogastroduodenoscopy (EGD) is a simple
procedure that is often performed with the patient
lightly sedated[1&2]. The procedure provides
significant information with high diagnostic
value upon which specific treatment can be given.
In certain cases, therapy can be administered
directly through the endoscope. Serious complications
rarely occur from upper gastrointestinal endoscopy
[3-5].
UGIE is indicated for the evaluation of patients
with upper abdominal symptoms that persist despite
an adequate trial of therapy, as well as, in
cases associated with other signs or symptoms
that suggest serious organic disease such as
weight loss, in patients who are over the age
of 50 years [6]. Upper GI endoscopy is also
indicated for the evaluation of dysphagia, odynophagia,
and Oesophageal reflux that is persistent or
recurrent despite adequate therapy, persistent
vomiting of an unknown cause, or diarrhea [6].
The procedure is also common for screening patients
for gastric cancer [7-9].
Gastrointestinal disorders are among the common
causes of visiting health care facilities in
Saudi Arabia and the number of patients attending
endoscopy units for various gastro symptoms
is increasing [10-13]. Dyspepsia was considered
among the most common indications for upper
gastrointestinal endoscopy [14-16], while other
causes are also overwhelming [17-19].
The objectives of this study were to identify
the common indications and findings on Upper
endoscopy in patients presenting to King Fahd
Central Hospital (KFCH) in Gizan, Southwest
Saudi Arabia, and to study the associations
between common endoscopic findings and some
selected demographic and clinical variables.
This was a retrospective study carried out
at King Fahad Central Hospital over a 11 year
period from 1994 to 2005. King Fahd Central
hospital is a tertiary hospital that serves
Jazan region which is populated with nearly
1.5 million people. The endoscopy unit provides
an open-access service and receives patients
from outpatient clinics and other hospitals
in the region. All patients (3287), age 12 years
and above referred for endoscopy unit were enrolled
in this study.
Standardized form (sheet) was used for extracting
data from medical record department that includes;
clinical data, demographic characteristics,
indications for UGIE and findings for all patients
undergoing upper endoscopy were recorded. Indications
for UGI E were classified as; upper gastrointestinal
bleeding; anemia; reflux symptoms heartburn
and/or regurgitation; dysphagia, weight loss,
anorexia, dyspepsia and other symptoms. In case
of multiple indications the predominant one
was chosen.
Data entry and statistical analyses were carried
out with SPSS 17. Descriptive statistics based
on frequency distributions and percentages were
used for presenting the results. Chi-square
tests/Fisher exact test were used to compare
categorical variables and to assess some associations;
two-proportion z-test was also utilized to compare
some proportions. Logistic regression model
was also used to evaluate factors associated
with the common findings of UGIE. A p- value
< 0.05 was considered to be statistically
significant.
As per international guidelines and KFCH endoscopy
guidelines, an informed written consent [20-21]
was obtained from all adults. An informed written
consent was obtained from guardians of all patients
less than 18 years enrolled, as per ethical
guidelines regulations in Saudi Arabia. Purpose,
potential risk and benefits of the endoscopy
have been communicated in Arabic language and
consent was documented for all participants.
The ethical approval for the current study was
obtained from the ethical committee at the Faculty
of Medicine, Jazan University. It should be
noted that the study was based on the secondary
data collected from the patient's files during
the study period, so it does not deal with any
personal data, since it was anonymous .
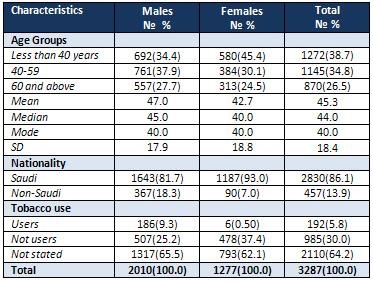
A
total
of
3287
UGIE's
were
performed
over
the
11
year
period
of
the
study.
Table
1
illustrates
some
background
characteristics
of
the
study
population.
The
mean
age
of
the
participants
was
45
years
(SD=18.4).
Around
38.7%
of
study
participants
were
less
than
40
years
old,
followed
by
34.8%
of
participants
who
were
in
the
age
group
40
to
59
years
old.
The
majority
of
study
participants
were
Saudi
86.1%,
compared
to
13.9%
who
were
non-Saudi.
Only
5.8%
of
study
subjects
reported
tobacco
use.
Male
participants
constituted
61.1%,
of
the
study
participants
while
those
females
were
38.9%.
Table
1:
Age
distribution,
nationality
and
Tobacco
use
among
study
participants
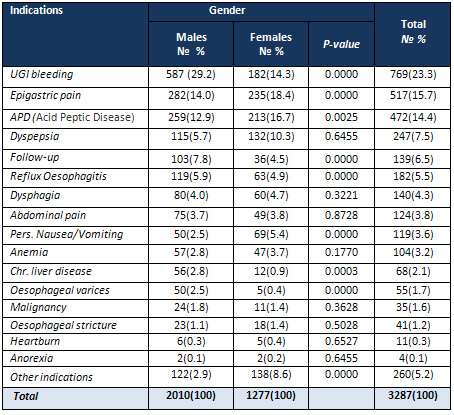
According
to
Table
2,
the
commonest
indications
for
endoscopy
among
study
participants
were
UGI
bleeding
(23.3%),
with
a
significant
difference
between
males
and
females
(p-value
=0.000),
(29.2%)
and
(14.3%)
respectively.
Epigastric
pain
was
the
second
indication
(15.7%)
also
with
a
significant
difference
between
male
and
female
patients
(p-value=0.000).
Acid
Peptic
Disease
(APD)
was
the
third
indication
for
UGIE
(14.4%),
followed
by
Dyspepsia
(7.5%)
and
regular
follow-up
(6.5%).
Other
causes
were
Reflux
Oesophagitis
(5.5%),
Dysphagia
(4.3%),
Abdominal
pain
(3.8%),
Pers.
Nausea/Vomiting(3.6%)
and
Anemia
(3.2%).
Table
2:
Causes
of
referral
of
the
studied
patients
to
the
upper
endoscopy
unit
according
gender
Table
3
presents
results
on
findings
of
upper
GI
endoscopy
among
the
studied
patients
according
to
gender
and
age
groups.
The
table
suggests
that
endoscopic
diagnoses
revealed
normal
findings
in
21.3%
of
patients.
Normal
findings
for
females
were
(31.0%)
significantly
higher
than
for
male
patients
(15.5%),
p-value
=
0.000.
Normal
findings
also
differ
significantly
according
to
age
groups
(p-value
=0.000),
and
show
a
decreasing
trend
with
increase
in
patient's
age.
Table
3
further
confirmed
that
pattern
of
endoscopic
diagnoses
shows
the
persistence
of
three
common
diseases;
Oesoph
Varices
(15.2%),
Gastritis(14.0%)
and
Oesophagitis(10%).
Oesoph.
Varices
was
significantly
higher
among
males
than
females,
and
also
significantly
different
among
the
three
different
age
groups
(p-value
=0.0000).
Gastritis
increases
with
increase
in
age
but
with
no
significant
differences
between
the
different
three
age
groups
and
gender.
Regarding
the
other
findings,
Duodenal
Ulcer
was
diagnosed
in
(9%)
of
the
patients
and
was
significantly
higher
in
males
than
females.
Gastric
Ulcer
disease
was
diagnosed
in
only
(3.7%)
of
the
patients.
Click
here
for
Table
3:
Findings
of
upper
endoscopy
among
the
studied
patients
according
to
gender
and
age
groups
The
results
of
logistic
regression
analyses
for
potential
risk
factors
of
three
common
endoscopic
findings
are
shown
in
Table
4.
The
analysis
revealed
that
gender,
and
patient's
age
was
associated
with
a
significantly
high
risk
of
Oesoph.
Varices
(OR=3.43
and
1.95
respectively
and
P-value<
0.001
for
all).
The
table
also
suggested
that
the
most
important
independent
predictors
of
Gastritis
were
patients'
age,
smoking
status
and
NSAID
use
(OR
=
1.36,
12.8,
2.786
and
4.284
respectively,
p-value<
0.05
for
all
coefficients).
None
of
the
variables
mentioned
in
the
table
were
a
significant
predictor
of
Oesophagitis
(p-value>0.05
for
all).
Click
here
for
Table
4:
Logistic
Regression
Analyses
for
potential
risk
factors
of
common
UGI
findings
among
the
study
patients
Gastrointestinal
(GI)
diseases
are
sources
for
substantial
morbidity
and
mortality
in
developing
as
well
as
in
developed
countries
[22].
Gastrointestinal
disorders
are
among
the
common
causes
of
visiting
health
care
facilities
in
Saudi
Arabia
[10-13].
These
types
of
diseases
affect
patients'
quality
of
life;
cause
a
significant
reduction
in
work
productivity
and
increased
economic
burden
[23&24].
This
is
the
first
study
that
has
dealt
with
UGI
E
in
Gizan
region.
Previously
published
work
on
UGI
endoscopy
in
Gizan
investigated
Barrett's
oesophagus
and
oesophageal
cancer
[25].
The
present
study
attempted
to
study
the
common
indications
and
findings
of
upper
endoscopy
in
patients
in
Gizan
patients
presenting
to
King
Fahd
Central
Hospital.
A
total
of
3287
UGI
endoscopy
were
performed
over
the
11
year
period
of
the
study.
The
results
of
the
study
suggested
that
UGI
bleeding
was
the
indication
for
UGIE
in
the
vast
majority
of
our
patients.
Such
a
high
proportion
has
not
been
reported
before
by
the
studies
conducted
in
KSA
[26,
27],
while
a
similar
trend
can
be
observed
from
other
West
African
and
East
African
studies
[28-29].
From
this
study,
the
next
most
common
indication
for
UGI
is
Epigastric
pain,
which
is
also
different
from
studies
conducted
in
other
parts
of
KSA[26,
27].
The
differences
in
the
commonest
indication
may
be
due
to
differences
in
the
terminologies
used.
Epigastric
pain
is
localized
to
the
region
of
the
upper
abdomen.
It
is
a
common
symptom
of
gastroesophageal
reflux
disease
(GERD)
or
heartburn.
On
the
other
hand
Acid
Peptic
Disease
(APD)
was
reported
as
the
third
indication
for
undergoing
UGIE.
APD
is
a
collective
term
used
to
include
many
conditions
such
as
gastro-esophageal
reflux
disease
(GERD),
gastritis,
gastric
ulcer,
duodenal
ulcer,
esophageal
ulcer
and
Zollinger
Ellison
Syndrome
(ZES).
Other
common
reasons
for
UGIE
among
our
patients
were
Dyspepsia,
Reflux
Oesophagitis,
dyspepsia
GERD
symptoms,
recurrent
vomiting
and
anemia.
Only
1.6%
of
our
patients
underwent
UGIE
for
Malignancy.
Although
Dyspepsia
is
less
encountered
in
our
studies,
it
accounts
for
15-77.5%
of
indications
for
UGIE
in
Saudi
Arabia
and
other
studies
elsewhere
[26,
30-34].
This
study
documented
three
common
diseases
reported
by
upper
endoscopy
procedures
which
are;
OesophVarices,
Gastritis
and
Oesophagitis.
The
results
suggest
that
esophageal
disease
is
common
in
Jazan
region.
Other
studies
in
Saudi
Arabia
indicate
the
low
prevalence
of
such
diseases
[12,26].
The
finding
that
the
prevalence
of
esophageal
varices
in
Gizan
differs
from
other
parts
of
Saudi
Arabia
[26]
draws
question
whether
it
is
linked
to
schistosomiasis,
which
may
be
the
underlying
cause
of
esophageal
varices
in
the
region,
during
the
study
time.
Similar
prevalence
was
reported
in
Sudan
in
which
schistosomiasis
is
prevalent
[35].
Suliman
et
al,
2010
attributed
the
increase
of
esophageal
disorders
to
the
changes
in
life
style
and
nutritional
habits
in
Saudi
Arabia[33].
Gastritis
is
a
well
known
heterogeneous
pathological
condition
that
is
responsible
for
the
incidence
of
many
gastrointestinal
diseases.
Literature
suggests
that
the
prevalence
of
gastritis
among
adults
in
the
Western
world
is
estimated
at
62%[36].
In
the
present
study,
Gastritis
was
the
commonest
pathology
reported
in
our
patients
with
prevalence
of
14%,
which
is
similar
to
other
studies
in
Saudi
and
other
Arabian
countries
[12,26,
35].
The
difference
between
our
results
and
western
countries'
prevalence
regarding
Gastritis
may
be
attributed
to
life
style
and
alcohol
use,
which
is
not
prevalent
in
Saudi
Arabia.
In
the
present
study
normal
endoscopy
was
reported
more
commonly
in
females
(31.2%)
as
compared
to
males
(15.3%)
showing
that
more
females
suffer
from
gastrointestinal
symptoms
in
our
setup.
Although
the
rate
of
normal
endoscopy
is
similar
to
other
Saudi
studies
conducted
during
the
past
20
years
[10-12],
it
calls
for
more
in-depth
investigation,
when
compared
to
more
recent
Saudi
and
regional
studies
[26&35].
In
this
article
an
effort
was
made
to
document
the
reasons
for
and
outcome
of
upper
gastrointestinal
endoscopy
in
Gizan
region
for
the
first
time.
The
limitations
of
this
study
are
that
subjects
were
studied
in
a
single
hospital
only.
In
addition,
the
fact
that
the
study
was
based
on
a
retrospective
study
design
may
not
allow
for
proper
causal
inferences
and
study
variables
were
limited
to
what
was
available
in
patients'
files.
In
conclusion
the
results
of
the
study
suggested
that
UGIE
bleeding
was
the
main
indication
for
UGIE
in
the
vast
majority
of
our
patients.
In
addition
to
that
three
common
diseases;
Oesophageal
Varices,
Gastritis
and
Oesophagitis
were
the
main
findings
of
the
UGIE
among
the
study
population.
Preventive
measures
should
be
adopted
to
cope
with
the
situation
and
to
prevent
complications
of
esophageal
and
gastritis
diseases
among
the
Jazan
population.
Abbreviations:
| KSA |
Kingdom
of
Saudi
Arabia |
| UGIE |
Upper
gastrointestinal
endoscopy |
| GI |
Gastrointestinal
|
| EGD |
Oesophagogastroduodenoscopy |
| KFCH |
King
Fahad
Central
Hospital
|
| APD |
Acid
Peptic
Disease |
| Oesoph |
Oesophageal |
| SD |
Standard
Deviation |
| HG |
Hypertensive
gastropathy
|
| GERD |
Gastro-esophageal
reflux
disease |
| ZES |
Zollinger
Ellison
Syndrome |
| CI |
Confidence
Interval |
| SPSS |
Statistical
Package
for
Social
Sciences |
| NSAIDS |
Nonsteroidal
anti-inflammatory
drugs |
| GE.
J. |
Gastroesophageal
Junction |
Acknowledgement:
I
would
like
to
thank
the
nursing
and
medical
staff
of
the
endoscopic
unit
of
the
King
Fahad
Central
Hospital,
Jazan
Region
KSA.
1.
Cotton
PB,
Hawes
RH,
Barkun
A,
et
al.
Excellence
in
endoscopy:
toward
practical
metrics.
GastrointestEndosc
2006;
63:286.
2.
Bjorkman
DJ,
Popp
JW
Jr.
Measuring
the
quality
of
endoscopy.
GastrointestEndosc
2006;
63:S1.
3.
Silvis
SE,
Nebel
O,
Rogers
G,
et
al.
Endoscopic
complications.
Results
of
the
1974
American
Society
for
Gastrointestinal
Endoscopy
Survey.
JAMA
1976;
235:928.
4.
Geraci
G,
Pisello
F,
Modica
G,
et
al.
Complications
of
elective
esophago-gastro-duodenoscopy
(EGDS).
Personal
experience
and
literature
review].
G
Chir
2009;
30:502.
5.
Wolfsen
HC,
Hemminger
LL,
Achem
SR,
et
al.
Complications
of
endoscopy
of
the
upper
gastrointestinal
tract:
a
single-center
experience.
Mayo
ClinProc
2004;
79:1264.
6.
American
Society
for
Gastrointestinal
Endoscopy.
Appropriate
use
of
gastrointestinal
endoscopy.
GastrointestEndosc
2000;
52:
831-7.
7.
Cappell,
M.
S.,
&Friedel,
D.
The
role
of
esophagogastroduodenoscopy
in
the
diagnosis
and
management
of
upper
gastrointestinal
disorders.
Medical
Clinics
of
North
America,
2002;
86(6),
1165-1216.
8.
ASGE
Standards
of
Practice
Committee,
Evans
JA,
Early
DS,
et
al.
The
role
of
endoscopy
in
Barrett's
esophagus
and
other
premalignant
conditions
of
the
esophagus.
GastrointestEndosc
2012;
76:1087.
9.
Hirota
WK,
Zuckerman
MJ,
Adler
DG,
et
al.
ASGE
guideline:
the
role
of
endoscopy
in
the
surveillance
of
premalignant
conditions
of
the
upper
GI
tract.
GastrointestEndosc
2006;
63:570.
10.
Ayoola
EA,
Al-Rashed
RS,
Al-Mofleh
IA,
Al-
Faleh
FZ,
Laajam
M.
Diagnostic
yield
of
upper
gastrointestinal
endoscopy
in
relation
to
age
and
gender:
a
study
of
10112
Saudi
patients.
Hepatogastroenterology
1996;
43:
409-15.
11.
Satti
MB,
Twum-Danso
K,
Al-Freihi
HM,
Ibrahim
EM,
Al-Gindan
Y,
Al-Quorain
A,
et
al.
Helicobacter
pylori-associated
upper
gastrointestinal
disease
in
Saudi
Arabia:
a
pathologic
evaluation
of
298
endoscopicbiopsies
from
201
consecutive
patients.
Am
J
Gastroenterol
1990;
85:
527-34.
13.
12.
Al-Quorain
A,
Satti
MB,
Al-Hamdan
A,
Al-Gassab
G,
Al-Freihi
H,
Al-Gindan
Y.
Pattern
of
upper
gastrointestinal
disease
in
the
eastern
province
of
Saudi
Arabia:
endoscopic
evaluation
of
2982
patients.
Trop
Geogr
Med
1991;
43:
203-8.
13.
Al-ShehriAM,
Al-Knawy
B,
Al-Jaber
K.
Use
of
a
simple
questionnaire
developed
by
the
American
College
of
gastroenterology
to
determine
prevalence
of
GERD
among
a
community-based
population
in
Saudi
Arabia.
Saudi
J
Gastroenterology
2003;
9:
49.
14.
Cooper
GS.
Indications
and
contraindications
for
upper
gastrointestinal
endoscopy.
GastrointestEndoscClin
N
Am
1994;
4:
439-454
15.
Taye
M,
Kassa
E,
Mengesha
B,
Gemechu
T,
Tsega
E
Upper
gastrointestinal
endoscopy:
a
review
of
10,000
cases.
Ethiop
Med
J
2004;
42:
97-107
[PMID:
16895026].
16.
Olokoba
AB,
Olokoba
LB,
Jimoh
AA,
Salawu
FK,
Danburam
A,
Ehalaiye
BF.
Upper
gastrointestinal
tract
endoscopy
indications
in
northern
Nigeria.
J
Coll
Physicians
Surg
Pak
2009;
19:
327-328.
17.
Tedesco
FJ,
Endoscopy
in
the
evaluation
of
patients
with
upper
gastrointestinal
symptoms:
indications,
expectations,
and
interpretation.
J.Clin.
Gastro
enterol.
1980;
3
(suppl
2):
67-71.
7.
18.
Health
and
public
committee,
American
College
of
Physicians,
Philadelphia,
Pennsylvania.,
Clinical
competence
in
diagnostic
OGD.
Annals
of
internal
Medicine
1987;
937-939.
8.
19.
The
working
party
of
the
clinical
services
committee
of
the
British
Society
of
gastro
enterology.
Provision
of
GI
endoscopy
and
relevant
services
for
district
general
hospital,
Gut
1991;
32:
95-100.
20.
Standards
of
Practice
Committee,
Zuckerman
MJ,
Shen
B,
et
al.
Informed
consent
for
GI
endoscopy.
GastrointestEndosc
2007;
66:213.
21.
Plumeri
PA.
Informed
consent
for
gastrointestinal
endoscopy
in
the
'90s
and
beyond.
GastrointestEndosc
1994;
40:379.
22.
Peery,
A.
F.,
Dellon,
E.
S.,
Lund,
J.,
Crockett,
S.
D.,
McGowan,
C.
E.,
Bulsiewicz,
W.
J.,
&Shaheen,
N.
J.
(2012).
Burden
of
gastrointestinal
disease
in
the
United
States:
2012
update.
Gastroenterology,
143(5),
1179-1187.?
23.
Kaji
M,
Fujiwara
Y,
Shiba
M,
et
al.
Prevalence
of
overlaps
between
GERD,
FD
and
IBS
and
impact
on
health-related
quality
of
life.
Journal
of
Gastroenterology
and
Hepatology
2010;
25(6):1151-1156.
24.
Barkun
A,
Leontiadis
G.
Systematic
Review
of
the
Symptom
Burden,
Quality
of
Life
Impairment
and
Costs
Associated
with
Peptic
Ulcer
Disease.
The
American
Journal
of
Medicine
2010;
123(4):
358-366.
25.
Gadour,
M.
O.,
&Ayoola,
E.
A.
(1998).
Barrett's
oesophagus
and
oesophageal
cancer
in
Saudi
Arabia.
Tropical
gastroenterology:
official
journal
of
the
Digestive
Diseases
Foundation,
20(3),
111-115.
26.
Al-Romaih,
W.
R.,
&
Al-Shehri,
A.
M.
(2006).
Appropriateness
of
upper
gastrointestinal
endoscopy
referrals
from
primary
health
care.
Annals
of
Saudi
medicine,
26(3),
224.?
27.
Azzam,
N.
A.,
Almadi,
M.
A.,
Alamar,
H.
H.,
Almalki,
L.
A.,
Alrashedi,
R.
N.,
Alghamdi,
R.
S.,
&
Al-hamoudi,
W.
Performance
of
American
Society
for
Gastrointestinal
Endoscopy
guidelines
for
dyspepsia
in
Saudi
population:
Prospective
observational
study.
World
journal
of
gastroenterology:
WJG,
2015;
21(2),
637.
28.
Khurram
M,
Kharr
HT,
Hassan
Z,
Umar
M,
Javed
S,
Asghar
T,
et
al.
A
12years
audit
of
upper
gastrointestinal
endoscopic
procedures.
J
Coll
Physician
Surg
Pak
2003
Jun;13(6):321-314.
29.
Taye
M,
Kassa
E,
Mengesha
B,
Gemechu
T,
Tsega.
Upper
gastrointestinal
endoscopy:
a
review
of
10,000
cases.
Ethiop
Med
J.2004;42(2):97-107.
30.
Jones
RH,
Lydeard
SE,
Hobbs
FD,
Kenkre
JE,
Williams
EI,
Jones
SJ,
et
al.
Dyspepsia
in
England
and
Scotland.
Gut.
1990;31:401-5.
31.
Knill-Jones
RP.
Geographical
differences
in
the
prevalence
of
dyspepsia.
Scand
J
Gastroenterol
Suppl.1991;182:17-24.
32.
Talley
NJ,
Silverstein
MD,
Agreus
L,
Nyren
O,
Sonnenberg
A,
Holtmann
G.
AGA
technical
review:
Evaluation
of
dyspepsia.
American
Gastroenterological
Association.
Gastroenterology.
1998;114:582-95.
33.
Al-Humayed,
S.
M.,
Mohamed-Elbagir,
A.
K.,
Al-Wabel,
A.
A.,
&
Argobi,
Y.
A.
The
changing
pattern
of
upper
gastro-intestinal
lesions
in
southern
Saudi
Arabia:
an
endoscopic
study.
Saudi
journal
of
gastroenterology:
official
journal
of
the
Saudi
Gastroenterology
Association,
2010;
16(1),
35.
34.
Zagari,
R.
M.,
Law,
G.
R.,
Fuccio,
L.,
Cennamo,
V.,
Gilthorpe,
M.
S.,
Forman,
D.,
&
Bazzoli,
F.
Epidemiology
of
functional
dyspepsia
and
subgroups
in
the
Italian
general
population:
an
endoscopic
study.
Gastroenterology
2010;
,138(4),
35.
Elhadi,
A.
A.,
Mirghani,
H.
O.,
Merghani,
T.
H.,
Mohammed,
O.
S.,
&
Eltoum,
H.
A
Pattern
of
Endoscopic
Findings
of
Upper
Gastrointestinal
Tract
in
Omdurman
Teaching
Hospital,
Sudan.
Sudan
Journal
of
Medical
Sciences,
2014;
9(2),
71-74.
36.
R.
J.
L.
F.
Loffeld,
B.
Liberov,
and
P.
E.
P.
Dekkers,
"The
changing
prevalence
of
upper
gastrointestinal
endoscopic
diagnoses:
a
single-centre
study,"
The
Netherlands
Journal
of
Medicine,
vol.
70,
no.
5,
pp.
222-226,
2012.
|

