To
promote
utilization
of
national
medical
research'
recommendations
among
health
policy
makers.
1.
To
identify
enabling
factors
for
utilization
of
national
medical
research'
recommendations
among
MOH
health
policy
makers
in
Jeddah
city,
KSA
2010.
2.
To
determine
barriers
among
MOH
health
policy
makers
toward
utilization
of
national
medical
research'
recommendations
in
Jeddah
city,
KSA
2010
Health
policy-makers
have
been
the
focus
of
studies.
Some
can
involve
health
policy-makers,
for
example
in
mental
health,
being
shown
research
papers
describing
evaluations
of
programmes
and
then
asked
how
useful
they
would
find
such
research.
Others
examine
the
policy-makers'
use
of
research
in
general.(9)
In
Canada
in
1999
one
study
interviewed
25
executive
directors
and
held
a
focus
group
with
a
group
of
other
directors
to
examine
the
use
and
transfer
of
research
in
these
organizations.
A
number
of
central
issues
were
identified
by
the
directors
that
affect
the
contribution
of
research
to
the
delivery
of
their
programs
and
services.
A
conceptual
model
for
developing
'locally-based
research
transfer'
was
subsequently
outlined
that
could
serve
as
the
basis
for
enhanced
research
use
and
research
transfer
in
other
local
area
contexts.(10)
In
Mexico
in
1999
the
results
of
a
descriptive
study
of
the
relationship
between
health
research
and
policy
in
four
vertical
programmes
(AIDS,
cholera,
family
planning,
immunization)
were
reported.
67
researchers
and
policy-makers
from
different
institutions
and
levels
of
responsibility
were
interviewed.
Then
interviewee
responses
looking
for
factors
that
promoted
or
impeded
exchanges
between
researchers
and
policy-makers
were
analyzed.
These
were,
in
turn,
divided
into
emphases
on
content,
actors,
process,
and
context.
Many
of
the
promoting
factors
resembled
findings
from
studies
in
industrialized
countries.
Some
important
differences
across
the
four
programmes,
which
also
distinguish
them
from
industrialized
country
programmes,
included
extent
of
reliance
on
formal
communication
channels,
role
of
the
mass
media
in
building
social
consensus
or
creating
discord,
levels
of
social
consensus,
role
of
foreign
donors,
and
extent
of
support
for
biomedical
versus
social
research.
Various
ways
were
recommended
to
increase
the
impact
of
research
on
health
policy-making
in
Mexico.
Some
of
the
largest
challenges
include
the
fact
that
researchers
are
but
one
of
many
interest
groups,
and
research
but
one
input
among
many
equally
legitimate
elements
to
be
considered
by
policy-makers.
Another
important
challenge
in
Mexico
is
the
relatively
small
role
played
by
the
public
in
policy-making.
Further
democratic
changes
in
Mexico
may
be
the
most
important
incentive
to
increase
the
use
of
research
in
policy-making.(19)
In
Poland
in
1999
a
national
postal
survey
was
conducted
and
supplemented
with
information
collected
during
focus
groups,
semi-structured
interviews
and
through
analysis
of
relevant
policy
documents.
The
main
aim
of
the
described
study
was
to
obtain
data
describing
the
needs,
preferences
and
limitations
of
healthcare
managers
as
information
users,
and
to
identify
environmental
factors
influencing
their
information
behaviour.
The
target
population
included
hospital
chief
executives,
medical
directors,
head
nurses
and
directors
of
the
institutions
responsible
for
health
services
planning
and
purchasing.
Target
institutions
were
drawn
systematically
from
official
lists,
stratified
by
regions
of
the
country
and
hospital
reference
level.
The
interviews
were
conducted
with
primary
care
unit
managers
and
with
Ministry
of
Health
officials.
National
health
strategy
and
directives,
cost-effectiveness
analyses
of
interventions
and
clinical
practice
guidelines
emerged
as
information
of
primary
importance
to
respondents.
The
main
barriers
to
effective
information
behavior
were
found
to
be:
attitudes
towards
research
activity,
lack
of
appropriately
processed
data,
lack
of
skills
enabling
information
seeking
and
appraisal,
inappropriate
format
of
publications,
ineffective
dissemination
of
information
and
absence
of
services
facilitating
access
to
evidence.
The
current
information
environment
of
healthcare
managers,
together
with
their
attitude
towards
information
and
deficiencies
in
information
skills,
appear
to
serve
as
a
barrier
to
evidence-based
practice
in
the
Polish
healthcare
system.(20)
In
2002
,
physicians
from
secondary
and
tertiary
hospitals
in
six
cities
located
in
China,
Thailand,
India,
Egypt
and
Kenya
were
enrolled
in
a
cross-sectional
questionnaire
survey.
The
primary
outcome
measures
were
scores
on
a
Likert
scale
reflecting
stated
likelihood
of
changing
clinical
practice
depending
on
the
source
of
the
research
or
its
publication.
Results
revealed
that
overall,
local
research
and
publications
were
most
likely
to
effect
change
in
clinical
practice,
followed
by
North
American,
European
and
regional
research/publications
respectively,
although
there
were
significant
variations
between
countries.
The
impact
of
local
and
regional
research
would
be
greater
if
the
perceived
research
quality
improved
in
those
settings.
It
was
concluded
that
conducting
high
quality
local
research
is
likely
to
be
an
effective
way
of
getting
research
findings
into
practice
in
developing
countries.(11)
In
2004,
a
survey
of
more
than
550
policy-makers
and
almost
1,900
researchers
in
13
low-
and
middle-income
countries
found
that,
on
average,
a
greater
proportion
of
policy-makers
than
researchers
reported
that
more
resources
should
be
spent
on
health
systems
research
such
as
health
policy,
service
delivery,
financing
and
surveillance
as
the
best
means
of
meeting
the
objectives
of
the
national
health
research
system.(12)
In
2007,
in
Mali,
a
study
of
the
selection
and
updating
of
Mali's
national
essential
medicines
list
was
undertaken
using
qualitative
methods.
In-depth
semi-structured
interviews
and
a
natural
group
discussion
were
held
with
national
policy-makers,
most
specifically
members
of
the
national
commission
that
selects
and
updates
the
country's
list.
The
resulting
text
was
analyzed
using
a
phenomenological
approach.
A
document
analysis
was
also
performed.
Results
showed
several
factors
emerged
from
the
textual
data
that
appear
to
be
influencing
the
utilization
of
health
research
findings
for
these
policy-makers.
These
factors
include:
access
to
information,
relevance
of
the
research,
use
of
research
perceived
as
a
time
consuming
process,
trust
in
the
research,
authority
of
those
who
presented
their
view,
competency
in
research
methods,
priority
of
research
in
the
policy
process,
and
accountability.
It
was
concluded
that
improving
the
transfer
of
research
to
policy
will
require
effort
on
the
part
of
researchers,
policy-makers,
and
third
parties.
This
will
include:
collaboration
between
researchers
and
policy-makers,
increased
production
and
dissemination
of
relevant
and
useful
research,
and
continued
and
improved
technical
support
from
networks
and
multi-national
organizations.
Policymakers
from
developing
countries
will
then
be
better
equipped
to
make
informed
decisions
concerning
their
health
policy
issues.
(5)
Up
to
the
researcher's
knowledge
there
is
no
similar
study
in
KSA,
hence
our
study
will
be
of
great
importance.
3.1
Study
Area:
Jeddah
is
a
Saudi
city
located
in
the
middle
of
the
Eastern
coast
of
the
Red
Sea
known
as
the
'Bride
of
the
Red
Sea'
and
is
considered
the
economic
and
tourism
capital
of
the
country.
Its
population
is
estimated
around
3.4
million
and
it
is
the
second
largest
city
after
Riyadh.(16)
The
study
was
conducted
in
Jeddah
Health
Affairs
involving
all
governmental
and
non
governmental
health
institutions.
Governmental
health
institutions
included
MOH
(Ministry
Of
Health)
hospitals
(n=
9)
plus
PHCC
(
Primary
Health
Care
Center)
sectors
(n=
7)
each
supervisory
sector
includes
6-7
centers
.While
non-governmental
health
institutions
included
all
private
hospitals
(n=31)
and
private
dispensaries
(n=181).
(data
were
obtained
from
Jeddah
Health
Affairs)
3.2
Study
Population:
Target
population
was
constituted
of
those
who
fulfill
definition
of
policy
makers
(individuals
responsible
for
the
development
of
policy
and
supervision
of
execution
of
plans
and
functional
operations).
Governmental:
-
PHCCs:
7
supervisory
sectors.
-
Hospitals:
9
hospitals
Private:
-
In
private
hospitals:
all
general
managers
and
medical
directors
-
In
private
dispensaries:
medical
directors.
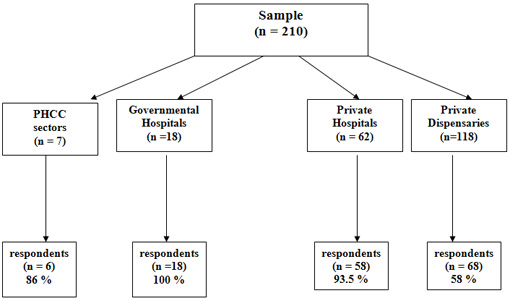
3.3
Study
Sample:
•
Sector
supervisors
(n=7)
•
General
managers
&
medical
directors
in
MOH
governmental
hospitals
(9*2)
(n=18)
•
Private
hospitals
(31*2)
(n=62)
•
Medical
directors
in
private
dispensaries
(n=118)
So,
total
was
210
after
adding
5
administrative
directors
at
Jeddah
Health
Affairs
to
the
population
sample.
3.4
Study
Design:
A
cross-sectional
descriptive
study.
3.5
Data
collection
tool:
Validated
questionnaire
published
in
several
studies(15),(17),(18)
for
administrators,
clinicians,
nurses
and
librarians
&
revised
by
epidemiologist
and
public
health
consultant
for
further
adaptation
and
modification
for
policy
makers.
It
was
bilingual
(2
versions
English
&
Arabic)
(see
appendix);
the
English
version
was
translated
into
Arabic
then
it
was
back
translated
to
ensure
lexical
equivalence.
The
questionnaire
included
3
parts:
Socio-demographic
data,
enabling
factors
and
barriers.
The
first
part
was
about
enabling
factors
of
utilization
of
research'
recommendations
(19
questions
plus
8
research
related
questions)
using
a
5
point
Likert
scale
in
which
5=strongly
agree
while
1=strongly
disagree;
the
second
part
was
about
barriers
to
utilization
of
research'
recommendations
(27
questions)
using
the
same
scale
and
the
third
part
included
socio-demographic
data
(7
items).
3.6
Data
collection
technique:
Self
administered
questionnaire
was
used
for
data
collection.
Questionnaires
were
distributed
by
the
researcher
and
3
well
trained
data
collectors
during
regular
day
working
hours
over
a
3
month
period
using
different
methods.
The
first
was
by
visiting
the
hospital
and
meeting
directly
with
the
Director
of
the
hospital
who
filled
out
the
form;
the
second
method
was
to
put
a
file
that
contains
a
form
with
a
letter
from
the
Health
Affairs
Director
and
return
at
a
later
date
to
receive
it
and
the
third
method
was
through
sending
the
form
via
fax
or
e-mail
attached
with
a
letter
after
talking
with
the
director
and
explaining
the
purpose
of
the
research
The
majority
of
data
were
collected
through
direct
meetings.
Regular
meetings
and
contact
between
researcher
and
data
collectors
and
monthly
written
reports
for
progress
of
data
collection
were
done.
All
the
data
were
verified
by
hand
then
were
coded
and
entered
into
a
personal
computer.
3.7
Data
entry
and
analysis:
Data
were
entered
and
analyzed
using
SPSS
version
16.
Categorical
variables
were
presented
as
frequency
and
percentage.
3.8
Pilot
study:
A
pilot
study
was
conducted
in
Makkah
among
10
health
policy
makers
from
different
health
institutions
to
test
the
validity
of
the
questionnaire.
Modifications
were
done
accordingly.
3.9
Ethical
considerations:
•
Written
permission
from
Joint
Program
of
Family
&
Community
Medicine
was
obtained
before
conduction
of
the
research.
•
Written
permission
from
the
concerned
authority
in
MOH
was
obtained
too.
•
Individual
consent
was
considered
as
a
prerequisite
for
data
collection.
It
was
written
on
the
front
page
of
the
questionnaire
that
answering
the
questionnaire
implied
agreement
to
participate
in
the
study).
•
All
information
was
kept
confidential
and
was
not
accessed
except
for
the
purpose
of
scientific
research
3.10
Budget:
The
research
is
self
funded.
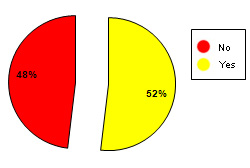
The
current
study
aims
at
identifying
enabling
factors
and
determining
barriers
among
health
policy
makers
toward
utilization
of
national
medical
research'
recommendations
in
Jeddah
Governorate.
Accordingly
the
respondents
were
210;
response
rate
is
shown
in
Figure
1
and
compensation
of
non
respondents
were
by
medical
directors
of
large
poly
clinics
and
administrative
directors.
Figure
1:
response
rate
of
the
participants
in
the
study
1.
Characteristics
of
the
study
group:
Demographic
characteristics
of
the
study
group
Table
1:
Demographic
characteristics
of
the
study
group
(n=210)
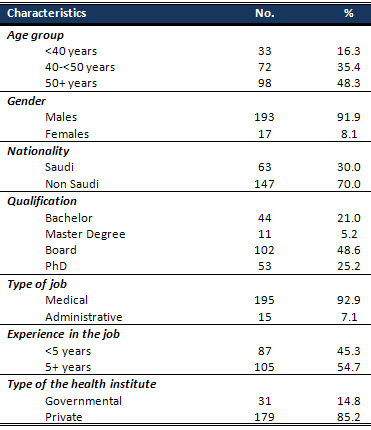
The
table
shows
that
the
majority
of
the
participants
170
(83.7%)
were
in
their
5th
decade
or
above,
and
the
overwhelming
majority
193
(91.9%)
are
males.
The
Saudis
constituted
63
(30%)
of
the
policy
makers
in
the
involved
health
institute,
and
those
who
have
postgraduate
qualifications
amounted
to
be
166
(79%)
who
have
mainly
Board
102
(48.6%)
or
PhD
degrees
53
(25.2%).
The
majority
of
the
participants
have
medical
jobs
195
(92.9)
and
slightly
more
than
one
half
of
them
105
(54.7%)
have
experience
in
their
job
of
five
years
or
more.
The
participants
in
the
governmental
health
institutes
accounted
for
31(14.8%).
Table
2:
Previous
and
current
participation
in
research
and
opinion
about
conduction
of
research
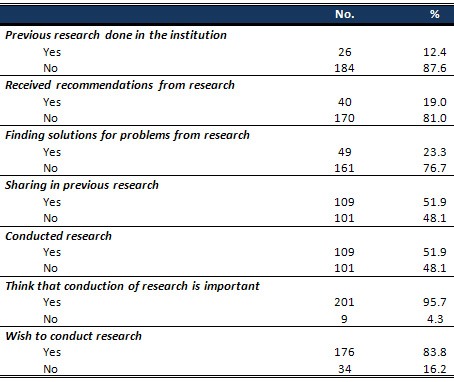
The
table
shows
that
only
12.4%
of
the
respondents
indicated
that
there
was
previous
research
conducted
in
their
institution
while
19%
addressed
that
they
received
recommendations
from
the
previously
conducted
research.
Moreover,
23.3%
pointed
out
that
they
find
solutions
for
their
problems
in
the
received
recommendations.
It
was
noted
that
51.9%
of
the
respondents
shared
in
previous
research,
and
an
equal
percentage
reported
that
they
conducted
research
(Figure
2).
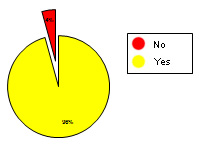
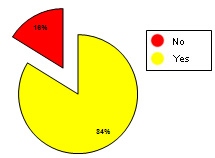
On
the
other
hand,
it
was
remarked
that
although
95.7%
of
the
respondents
believe
that
conduction
of
research
is
important
(Figure
3),
nevertheless,
a
lower
percentage
(83.8%)
of
them
expressed
that
they
wish
to
conduct
research
(Figure
4).
Figure
2:
Previous
research
done
in
the
institution
Figure
3:
Conducted
research
Figure
4:
Think
that
conduction
of
research
is
important
Figure
5:
Wish
to
conduct
research
Click
here
for
Table
3:
Agreement
of
the
respondents
to
the
items
representing
enabling
factors
for
research
The
table
demonstrates
the
agreement
of
the
participants
about
the
statements
representing
the
enabling
factors
for
research.
It
shows
that
the
majority
of
them
agree
about
the
research
quality
being
an
enabling
factor
(90%),
and
an
almost
equal
percentage
(91.1%)
agree
about
concern
in
biomedical
rather
than
social
research,
and
90.9%
agree
about
the
importance
of
specificity,
concreteness
and
cost
effectiveness.
Moreover,
it
was
found
that
95.2%
of
the
respondents
assert
their
agreement
about
the
importance
of
national
support
as
an
enabling
factor,
and
90.5%
pointed
to
the
formal
communications
in
addition
to
91%
who
addressed
political
stability
as
enabling
factors.
On
the
other
hand,
it
was
noted
that
the
great
majority
of
the
participants
(91.5%)
disagree
about
the
assumption
that
utilizing
research
findings
is
time
consuming.
Click
here
for
Table
4:
Agreement
of
the
respondents
to
the
items
representing
barriers
for
research.
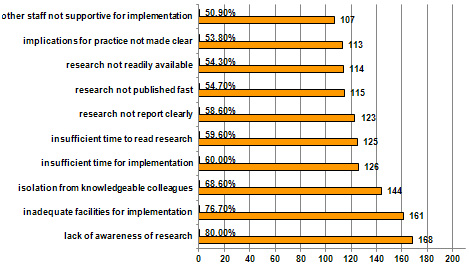
The
table
illustrates
the
response
of
the
participants
to
the
items
representing
barriers
for
conducting
research
arranged
in
descending
order
according
to
the
overall
agreement
for
each
item.
Based
on
this
ranking,
it
was
evident
that
the
top
ten
barriers
included
a
pile
of
situations
pertinent
to
the
staff
working
in
the
institute
such
as
lack
of
their
awareness
to
research,
being
isolated
from
knowledgeable
colleagues
with
whom
to
discuss
the
research
and
lack
of
support
from
other
staff
in
its
implementation.
The
other
pile
of
barriers
are
related
to
the
quality
of
the
research,
where
it
was
found
that
there
is
high
agreement
on
the
ambiguous
reporting
of
the
research,
being
not
readily
available,
vague
implication
on
practice
in
addition
to
late
publication
are
potential
barriers
for
conducting
research.
Moreover,
two
of
the
top
ten
barriers
are
conceptualized
around
the
time
factor,
where
it
was
found
that
60%
of
the
respondents
perceive
that
there
is
not
sufficient
time
on
the
job
to
implement
new
ideas,
in
addition
to
58.6%
who
see
that
there
is
not
sufficient
time
to
read
research.
Finally,
the
factor
which
is
related
to
the
institute
in
general
was
represented
by
the
availability
of
facilities,
where
it
was
found
that
76.7%
of
the
participants
consider
the
inadequate
facilities
in
the
institute
as
a
crucial
barrier
for
implementing
research.
On
the
other
hand,
it
was
remarked
that
the
least
potential
barriers
for
conducting
research
perceived
by
the
respondents
were
related
to
fine
details
of
the
research,
for
example:
difficulty
to
understand
statistical
analyses,
inadequacy
of
the
methodological
design
and
unjustified
conclusions
drawn
from
the
research.
Figure
6:
Agreement
of
the
respondents
to
the
items
representing
top
ten
barriers
for
research
conduction
Making
the
best
use
of
available
research
studies
is
a
priority
goal
in
most
countries,
developed
or
developing,
and
what
was
promising
in
our
study
was
that
the
majority
of
participants
had
a
positive
attitude
toward
research
conduction
although
little
research
was
conducted
by
participants
and
few
of
them
were
useful
in
practice
in
comparison
with
Polish
managers
where
only
15%
of
respondents
thought
that
research
results
had
significant
influence
on
practice
in
health
care,
and
only
3.2%
perceived
developments
in
scientific
knowledge
as
having
an
input
in
their
area
of
decision
making.(20)
Troslte
et
al(19)
looked
for
factors
that
promoted
or
impeded
exchanges
between
researchers
and
policy
makers.
These
were
in
turn
divided
into
emphasis
on
content,
actors,
process,
and
context.
They
finally
recommended
improving
communication
between
researchers
and
policy
makers
via
training
of
both
parties:
assisting
researchers
to
communicate
their
findings
in
an
understandable
and
stimulating
way,
or
synthesizing
policy
makers
on
the
usefulness
of
research
results
as
an
input
to
decision
making.
They
also
recommended
that
research
should
be
evaluated
in
terms
of
its
cost
and
effectiveness
before
being
considered
as
the
basis
for
a
policy
or
program.
However,
this
type
of
evaluation
is
still
underdeveloped
internationally.
(19)
While
in
a
Mali
study
(5)
the
factors
influencing
the
use
of
research
findings
were
Policy-makers'
access
to
information,
relevance
of
research
findings,
perception
that
utilizing
research
findings
is
time-consuming,
policy-makers'
competency
in
research
methods,
trust
policy-makers
place
on
research,
authority
of
those
who
present
their
view,
relative
importance
or
priority
of
research
findings
compared
with
other
sources
of
information
in
the
policy-process
and
uncertainty
of
who
is
responsible
or
accountable
for
accessing,
locating,
and
providing
research
findings
to
address
the
policy-decisions.
In
our
study
the
participants
point
of
views
were
comparable
except
for
the
perception
that
utilizing
research
findings
is
time-consuming,
where
the
majority
disagreed.
On
the
other
hand
two
of
the
top
ten
barriers
are
conceptualized
around
the
time
factor,
where
it
was
found
that
60%
of
the
respondents
perceive
that
there
is
not
sufficient
time
on
the
job
to
implement
new
ideas,
in
addition
to
58.6%
who
see
that
there
is
not
sufficient
time
to
read
research
and
this
could
be
explained
in
the
way
of
utilization
of
research
findings
will
outweigh
the
time
consumed
for
research
conduction
i.e
efficiency
will
mask
real
time
consuming.
Moreover,
it
was
found
that
the
other
top
barriers
included
a
pile
of
situations
pertinent
to
the
staff
working
in
the
institute
such
as
lack
of
their
awareness
to
research,
being
isolated
from
knowledgeable
colleagues
with
whom
to
discuss
the
research
and
lack
of
support
from
other
staff
in
its
implementation.
The
other
pile
of
barriers
are
related
to
the
quality
of
the
research,
where
it
was
found
that
there
is
high
agreement
on
that
the
ambiguous
reporting
of
the
research,
being
not
readily
available,
vague
implications
on
practice,
in
addition
to
late
publication,
are
potential
barriers
for
conducting
research.
Finally,
the
factor
which
is
related
to
the
institute
in
general
was
represented
by
the
availability
of
facilities,
where
it
was
found
that
76.7%
of
the
participants
consider
the
inadequate
facilities
in
the
institute
is
considered
as
a
crucial
barrier
for
implementing
research.
The
current
study
revealed
that
among
the
interviewed
health
policy-makers
there
was
a
gap
between
the
perceived
importance
of
the
research
from
one
side
and
its
conduction
and
utilization
of
its
recommendations
on
the
other
side.
The
reported
barriers
are
mainly
remediable
as
being
attributed
chiefly
to
modifiable
subjective
factors
driven
from
the
lack
of
knowledge
and
experience
about
research
methodology.
In
addition,
the
insufficient
time
perceived
as
a
barrier
reflects
the
vision
of
the
studied
institute
which
are
not
focusing
in
part
of
it
on
conduction
of
research
and
incorporating
it
in
its
plan
and
regular
routine
work.
•
Encouragement
of
conduction
of
research
in
different
health
institutions
through
real
and
pragmatic
support.
•
Incorporate
any
executive
directors,
planners
or
managers
who
are
subjected
to
trainer
course
for
administration
to
be
fortified
by
a
research
methodology
course
•
Deliberate
efforts
should
be
made
to
legislate
provision
of
incentives
for
research
implementation.
(1)
World
Health
Organization.
World
report
on
knowledge
for
better
health
strengthening
health
systems.
Geneva:
World
Health
Organization;
2004.
Available
from
URL
:
http://www.who.int/rpc/meetings/en/world_report_on_knowledge_for_better_health2.pdf
(2)
Hutchinson
AM,
Johnston
L.
Beyond
the
BARRIERS
Scale:
commonly
reported
barriers
to
research
use.
J
Nurs
Adm
2006
Apr;36(4):189-99.
(3)
Gagliardi
AR,
Fraser
N,
Wright
FC,
Lemieux-Charles
L,
Davis
D.
Fostering
knowledge
exchange
between
researchers
and
decision-makers:
exploring
the
effectiveness
of
a
mixed-methods
approach.
Health
Policy
2008
Apr;86(1):53-63.
(4)
Gilson
L,
McIntyre
D.
The
interface
between
research
and
policy:
experience
from
South
Africa.
Soc
Sci
Med
2008
Sep;67(5):748-59.
(5)
Albert
MA,
Fretheim
A,
Maiga
D.
Factors
influencing
the
utilization
of
research
findings
by
health
policy-makers
in
a
developing
country:
the
selection
of
Mali's
essential
medicines.
Health
Res
Policy
Syst
2007;5:2.
(6)
Titler
MG.
Methods
in
translation
science.
Worldviews
Evid
Based
Nurs
2004;1(1):38-48.
(7)
Bostrom
AM,
Kajermo
KN,
Nordstrom
G,
Wallin
L.
Barriers
to
research
utilization
and
research
use
among
registered
nurses
working
in
the
care
of
older
people:
Does
the
BARRIERS
Scale
discriminate
between
research
users
and
non-research
users
on
perceptions
of
barriers?
Implement
Sci
2008;3:24.
(8)
Innvaer
S,
Vist
G,
Trommald
M,
Oxman
A.
Health
policy-makers'
perceptions
of
their
use
of
evidence:
a
systematic
review.
J
Health
Serv
Res
Policy
2002
Oct;7(4):239-44.
(9)
Hanney
SR,
Gonzalez-Block
MA,
Buxton
MJ,
Kogan
M.
The
utilisation
of
health
research
in
policy-making:
concepts,
examples
and
methods
of
assessment.
Health
Res
Policy
Syst
2003
Jan
13;1(1):2.
(10)
Anderson
M,
Cosby
J,
Swan
B,
Moore
H,
Broekhoven
M.
The
use
of
research
in
local
health
service
agencies.
Soc
Sci
Med
1999
Oct;49(8):1007-19.
(11)
World
Health
Organization.
World
report
on
knowledge
for
better
health
strengthening
health
systems.
Geneva:
World
Health
Organization;
2004.
(12)
Page
J,
Heller
RF,
Kinlay
S,
Lim
LL,
Qian
W,
Suping
Z,
et
al.
Attitudes
of
developing
world
physicians
to
where
medical
research
is
performed
and
reported.
BMC
Public
Health
2003
Jan
16;3:6.
(13)
Medical
Dictionary
Online.
Available
from
URL:
http://www.online-medicaldictionary.org/omd.asp?q=POLICY+MAKER
(14)
Pakenham-Walsh
N,
Learning
from
one
another
to
bridge
the
"know-do
gap"
,BMJ
2004;329:1189
(13
November),
doi:10.1136/bmj.329.7475.1189
(15)
Albert
M,
Using
evidence
to
select
essential
medicines,
ESSENTIAL
MEDICINES
MONITOR
WHO,
2009
Nov(2)
(16)
Available
from
http://www.jeddah.gov.sa/English/jeddah/index.php
(17)
Afifi
M
1,
Bener
A,
Research
to
policy
in
the
Arab
world:
lost
in
translation,
Middle
East
Journal
of
Family
Medicine,
2007
Sep
;5(6)
(18)
Funk
SG,
Tornquist
EM,
and
Champagne
MT
,BARRIERS
AND
FACILITATORS
OF
RESEARCH
UTILIZATION
an
Integrative
Review
(19)
Trostle
J,
Brofman
M,
Langer
A.
How
do
researchers
influence
decision
makers?
Case
studies
of
Mexican
policies.
Health
Policy
and
Planning
1999;
14:103-114.
(20)
Niedzwiedzka
BM,
Barriers
to
evidence-based
decision
making
among
Polish
healthcare
managers.
Health
Serv
Manage
Res.
2003
May;16(2):106-15.
Click
here
for
pdf
of
English
and
Arabic
versions
of
Appendix

