|
|
 |
| ............................................................. |
|
October 2017 -
Volume 15, Issue 8
|
 |
|
View
this issue in pdf formnat - the issue
has been split into two files for downloading
due to its large size: FULLpdf
(12 MB)
Part
1 &
Part
2
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
........................................................
|
|
Original Contribution/Clinical Investigation
Immunity
level to diphtheria in beta thalassemia patients
DOI: 10.5742/MEWFM.2017.93048
[pdf
version]
Abdolreza Sotoodeh Jahromi, Karamatollah Rahmanian,
Abdolali Sapidkar, Hassan Zabetian, Alireza
Yusefi, Farshid Kafilzadeh, Mohammad Kargar,
Marzieh Jamalidoust,
Abdolhossein Madani
Genetic
Variants of Toll Like Receptor-4 in Patients
with Premature Coronary Artery Disease, South
of Iran
DOI: 10.5742/MEWFM.2017.93049
[pdf
version]
Saeideh Erfanian, Mohammad Shojaei, Fatemeh
Mehdizadeh, Abdolreza Sotoodeh Jahromi, Abdolhossein
Madani, Mohammad Hojjat-Farsangi
Comparison
of postoperative bleeding in patients undergoing
coronary artery bypass surgery in two groups
taking aspirin and aspirin plus CLS clopidogrel
DOI: 10.5742/MEWFM.2017.93050
[pdf
version]
Ali Pooria, Hassan Teimouri, Mostafa Cheraghi,
Babak Baharvand Ahmadi, Mehrdad Namdari, Reza
Alipoor
Comparison
of lower uterine segment thickness among nulliparous
pregnant women without uterine scar and pregnant
women with previous cesarean section: ultrasound
study
DOI: 10.5742/MEWFM.2017.93051
[pdf version]
Taravat Fakheri, Irandokht Alimohammadi, Nazanin
Farshchian, Maryam Hematti,
Anisodowleh Nankali, Farahnaz Keshavarzi, Soheil
Saeidiborojeni
Effect
of Environmental and Behavioral Interventions
on Physiological and Behavioral Responses of
Premature Neonates Candidates Admitted for Intravenous
Catheter Insertion in Neonatal Intensive Care
Units
DOI: 10.5742/MEWFM.2017.93052
[pdf
version]
Shohreh Taheri, Maryam Marofi, Anahita Masoumpoor,
Malihe Nasiri
Effect
of 8 weeks Rhythmic aerobic exercise on serum
Resistin and body mass index of overweight and
obese women
DOI: 10.5742/MEWFM.2017.93053
[pdf
version]
Khadijeh Molaei, Ahmad Shahdadi, Reza Delavar
Study
of changes in leptin and body mass composition
with overweight and obesity following 8 weeks
of Aerobic exercise
DOI: 10.5742/MEWFM.2017.93054
[pdf
version]
Khadijeh Molaei, Abbas Salehikia
A reassessment
of factor structure of the Short Form Health
Survey (SF-36): A comparative approach
DOI: 10.5742/MEWFM.2017.93088
[pdf version]
Vida Alizad, Manouchehr Azkhosh, Ali Asgari,
Karyn Gonano
Population and Community Studies
Evaluation
of seizures in pregnant women in Kerman - Iran
DOI: 10.5742/MEWFM.2017.93056
[pdf
version]
Hossein Ali Ebrahimi, Elahe Arabpour, Kaveh
Shafeie, Narges Khanjani
Studying
the relation of quality work life with socio-economic
status and general health among the employees
of Tehran University of Medical Sciences (TUMS)
in 2015
DOI: 10.5742/MEWFM.2017.93057
[pdf version]
Hossein Dargahi, Samereh Yaghobian, Seyedeh
Hoda Mousavi, Majid Shekari Darbandi, Soheil
Mokhtari, Mohsen Mohammadi, Seyede Fateme Hosseini
Factors
that encourage early marriage and motherhood
from the perspective of Iranian adolescent mothers:
a qualitative study
DOI: 10.5742/MEWFM.2017.93058
[pdf
version]
Maasoumeh Mangeli, Masoud Rayyani, Mohammad
Ali Cheraghi, Batool Tirgari
The
Effectiveness of Cognitive-Existential Group
Therapy on Reducing Existential Anxiety in the
Elderly
DOI: 10.5742/MEWFM.2017.93059
[pdf
version]
Somayeh Barekati, Bahman Bahmani, Maede Naghiyaaee,
Mahgam Afrasiabi, Roya Marsa
Post-mortem
Distribution of Morphine in Cadavers Body Fluids
DOI: 10.5742/MEWFM.2017.93060
[pdf
version]
Ramin Elmi, Mitra Akbari, Jaber Gharehdaghi,
Ardeshir Sheikhazadi, Saeed Padidar, Shirin
Elmi
Application
of Social Networks to Support Students' Language
Learning Skills in Blended Approach
DOI: 10.5742/MEWFM.2017.93061
[pdf
version]
Fatemeh Jafarkhani, Zahra Jamebozorg, Maryam
Brahman
The
Relationship between Chronic Pain and Obesity:
The Mediating Role of Anxiety
DOI: 10.5742/MEWFM.2017.93062
[pdf
version]
Leila Shateri, Hamid Shamsipour, Zahra Hoshyari,
Elnaz Mousavi, Leila Saleck, Faezeh Ojagh
Implementation
status of moral codes among nurses
DOI: 10.5742/MEWFM.2017.93063
[pdf
version]
Maryam Ban, Hojat Zareh Houshyari Khah, Marzieh
Ghassemi, Sajedeh Mousaviasl, Mohammad Khavasi,
Narjes Asadi, Mohammad Amin Harizavi, Saeedeh
Elhami
The comparison
of quality of life, self-efficacy and resiliency
in infertile and fertile women
DOI: 10.5742/MEWFM.2017.93064
[pdf version]
Mahya Shamsi Sani, Mohammadreza Tamannaeifar
Brain MRI Findings in Children (2-4 years old)
with Autism
DOI: 10.5742/MEWFM.2017.93055
[pdf
version]
Mohammad Hasan Mohammadi, Farah Ashraf Zadeh,
Javad Akhondian, Maryam Hojjati,
Mehdi Momennezhad
Reviews
TECTA gene function and hearing: a review
DOI: 10.5742/MEWFM.2017.93065
[pdf version]
Morteza Hashemzadeh-Chaleshtori, Fahimeh Moradi,
Raziyeh Karami-Eshkaftaki,
Samira Asgharzade
Mandibular
canal & its incisive branch: A CBCT study
DOI: 10.5742/MEWFM.2017.93066
[pdf
version]
Sina Haghanifar, Ehsan Moudi, Ali Bijani, Somayyehsadat
Lavasani, Ahmadreza Lameh
The
role of Astronomy education in daily life
DOI: 10.5742/MEWFM.2017.93067
[pdf
version]
Ashrafoalsadat Shekarbaghani
Human brain
functional connectivity in resting-state fMRI
data across the range of weeks
DOI: 10.5742/MEWFM.2017.93068
[pdf version]
Nasrin Borumandnia, Hamid Alavi Majd, Farid
Zayeri, Ahmad Reza Baghestani,
Mohammad Tabatabaee, Fariborz Faegh
International Health Affairs
A
brief review of the components of national strategies
for suicide prevention suggested by the World
Health Organization
DOI: 10.5742/MEWFM.2017.93069
[pdf
version]
Mohsen Rezaeian
Education and Training
Evaluating
the Process of Recruiting Faculty Members in
Universities and Higher Education and Research
Institutes Affiliated to Ministry of Health
and Medical Education in Iran
DOI: 10.5742/MEWFM.2017.93070
[pdf
version]
Abdolreza Gilavand
Comparison
of spiritual well-being and social health among
the students attending group and individual
religious rites
DOI: 10.5742/MEWFM.2017.93071
[pdf
version]
Masoud Nikfarjam, Saeid Heidari-Soureshjani,
Abolfazl Khoshdel, Parisa Asmand, Forouzan Ganji
A
Comparative Study of Motivation for Major Choices
between Nursing and Midwifery Students at Bushehr
University of Medical Sciences
DOI: 10.5742/MEWFM.2017.93072
[pdf
version]
Farzaneh Norouzi, Shahnaz Pouladi, Razieh Bagherzadeh
Clinical Research and Methods
Barriers
to the management of ventilator-associated pneumonia:
A qualitative study of critical care nurses'
experiences
DOI: 10.5742/MEWFM.2017.93073
[pdf version]
Fereshteh Rashnou, Tahereh Toulabi, Shirin Hasanvand,
Mohammad Javad Tarrahi
Clinical
Risk Index for Neonates II score for the prediction
of mortality risk in premature neonates with
very low birth weight
DOI: 10.5742/MEWFM.2017.93074
[pdf
version]
Azadeh Jafrasteh, Parastoo Baharvand, Fatemeh
Karami
Effect
of pre-colporrhaphic physiotherapy on the outcomes
of women with pelvic organ prolapse
DOI: 10.5742/MEWFM.2017.93075
[pdf
version]
Mahnaz Yavangi, Tahereh Mahmoodvand, Saeid Heidari-Soureshjani
The
effect of Hypertonic Dextrose injection on the
control of pains associated with knee osteoarthritis
DOI: 10.5742/MEWFM.2017.93076
[pdf
version]
Mahshid Ghasemi, Faranak Behnaz, Mohammadreza
Minator Sajjadi, Reza Zandi,
Masoud Hashemi
Evaluation
of Psycho-Social Factors Influential on Emotional
Divorce among Attendants to Social Emergency
Services
DOI: 10.5742/MEWFM.2017.93077
[pdf
version]
Farangis Soltanian
Models and Systems of Health Care
Organizational
Justice and Trust Perceptions: A Comparison
of Nurses in public and private hospitals
DOI: 10.5742/MEWFM.2017.93078
[pdf
version]
Mahboobeh Rajabi, Zahra Esmaeli Abdar, Leila
Agoush
Case series and Case reports
Evaluation
of Blood Levels of Leptin Hormone Before and
After the Treatment with Metformin
DOI: 10.5742/MEWFM.2017.93079
[pdf
version]
Elham Jafarpour
Etiology,
Epidemiologic Characteristics and Clinical Pattern
of Children with Febrile Convulsion Admitted
to Hospitals of Germi and Parsabad towns in
2016
DOI: 10.5742/MEWFM.2017.93080
[pdf
version]
Mehri SeyedJavadi, Roghayeh Naseri, Shohreh
Moshfeghi, Irandokht Allahyari, Vahid Izadi,
Raheleh Mohammadi,
Faculty development
The
comparison of the effect of two different teaching
methods of role-playing and video feedback on
learning Cardiopulmonary Resuscitation (CPR)
DOI: 10.5742/MEWFM.2017.93081
[pdf
version]
Yasamin Hacham Bachari, Leila Fahkarzadeh, Abdol
Ali Shariati
Office based family medicine
Effectiveness
of Group Counseling With Acceptance and Commitment
Therapy Approach on Couples' Marital Adjustment
DOI: 10.5742/MEWFM.2017.93082
[pdf
version]
Arash Ziapour, Fatmeh Mahmoodi, Fatemeh Dehghan,
Seyed Mehdi Hoseini Mehdi Abadi,
Edris Azami, Mohsen Rezaei
|
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| October 2017 -
Volume 15, Issue 8 |
|
|
Clinical Risk Index for
Neonates II score for the prediction of mortality
risk in premature neonates with very low birth
weight
Azadeh Jafrasteh (1)
Parastoo Baharvand (2)
Fatemeh Karami (3)
(1) Department
of Pediatrics, Lorestan University of medical
Sciences, Khorramabad, Iran.
(2) Assistant Professor, Department of Community
Medicine, Lorestan University of medical Sciences,
Khorramabad, Iran.
(3) BSc Student, Student Research Committee,
Lorestan University of medical Sciences, Khorramabad,
Iran.
Correspondence:
Parastoo Baharvand
School of medicine,
Lorestan University of Medical Sciences,
Khorramabad, Lorestan, Iran
Email:
Dr.baharvand@gmail.com
|
Abstract
Introduction: One
of the most common methods of identifying
neonatal mortality risk is the Clinical
Risk Index for Babies scoring system (CRIB-
II). The aim of this study is to investigate
the value of CRIB II scoring system in
prediction of mortality risk in premature
neonates with birth weight less than 1500
gr.
Materials and
methods: This descriptive-analytical
investigation was conducted on premature
neonates with very low birth weight (less
than 1500 g) and gestational age less
than 32 weeks who were hospitalized in
NICU of Shahid Madani Hospital of Lorestan
province (southwest of Iran) during a
two-year period (January 2013 to December
2015). These neonates were hospitalized
during the first 12 hours of life and
evaluated according to CRIB II scoring
system. After collecting and completing
information about patients, the data was
analyzed using SPSS software.
Findings:
Of a total 272 neonates, 160 neonates
(58.82%) died in the hospital. Mean scores
of CRIB II were 6.1±2.7 and 9.7±3.1
for survivor neonates and non-survivor
neonates respectively (PV<0.001). In
a survey for specificity and sensitivity
of CRIB II score in mortality prediction
of premature neonates with birth weight
lower than 1500 gr, it was observed that
almost 83% (CI=74-91) of neonatal mortalities
can be predicted.
Discussion and
conclusion: This study showed that
CRIB II index has higher value in prediction
of mortality in premature neonates with
very low birth weight.
Key words:
Premature neonates, Mortality risk, CRIB
II.
|
Very low birth weight (VLBW) infants, weighing
less than 1500 g at birth, represent about 1%
of all births but account for 50% of neonatal
deaths. Compared with infants weighing 2500
g or more, LBW infants are 40 times more likely
to die in the neonatal period; VLBW infants
have a 200-fold higher risk of neonatal death
[1-3].
Contrary to reduction of neonatal mortality
rate in recent years, the mortality rate of
low birth weight infants has not reduced dramatically.
In general, neonatal mortality is a hygiene
index and it has a direct connection with the
economic and social states of the countries.
A higher percentage of premature neonatal mortalities
occur in Neonatal Intensive Care Unit (NICU)
and definitely, periodic investigation about
the activities of these units can be effective
in mortality reduction of this sensitive age
range. To investigate and compare the activity
of NICU, the adjustment of treatment results
with primary state of the patient and disease
intensity in hospitalization time is vital.
Application of a tool that can identify an unwell
patient in early hours of hospitalization, can
be helpful for evaluation of the medical team
activities. So to this end, numerous scoring
systems have been developed in order to identify
emergency patients in early hospitalization
in NICU and before any kind of medical and curing
activities that the Clinical Risk Index for
Babies (CRIB), CRIB II, Score for Neonatal Acute
Physiology (SNAP), Score for Neonatal Acute
Physiology-Perinatal-Extension (SNAP-PE) and
Neonatal Therapeutic Interventions Scoring System
(NTISS) can be mentioned [4]. These scoring
systems are different in terms of the type and
the number of evaluated variables, and the type
of scoring. CRIB scoring system has application
in neonates with birth weight less than 1500
gr but SNAP can be used in all gestational ages
and all weights [4].
For more than a decade, a clinical risks scoring
system has been applied to evaluate the neonate’s
state and their mortality rate in NICU of the
hospitals. Application of an index which is
less affected by other interruptive indexes
like steroid prophylaxis and to have more reliable
results is essential. CRIB scoring system is
comprised of 6 variables: birth weight, gestational
age, congenital anomalies, minimum and maximum
breathing oxygen percentage and maximum Base
deficiency information that are investigated
during the first 12 hours after hospitalization.
In CRIB II scoring system, only 5 variables
(birth weight, gestational age, neonate sex,
maximum Base deficiency, baby’s temperature
at hospitalization time) are used to evaluate
the premature neonates. These scoring systems
have predicting values in determination of neonate
mortality rates but there is no use for them
in morbidity prediction of neonates [1, 4].
Neonatal mortality rate is affected by NICU
facilities and the numbers of nurses. Most researchers
believe that CRIB II scoring system has higher
value for prediction of hospital premature neonatal
mortality with birth weight lower than 1500
gr in comparison to weight and pregnancy age
or both. Since all related variables are practical
in our occasion, CRIB II scoring system was
chosen to investigate the premature neonates.
This study is for evaluation of CRIB II scoring
system in prediction of neonatal mortality rate
at NICU ward of Shahid Madani hospital, Khorramabad,
Iran.
In this descriptive analytical study that was
carried out from January 2013 to December 2015
(two years) in NICU of Shahid Madani hospital
(Khorramabad, Lorestan province), after obtaining
permission from the ethics committee to do the
study in vulnerable groups, informed written
consent was taken from the parents. The study
population included all live-born neonates with
a birth-weight of 1500 gr and/or gestational
age 32 weeks. Exclusion criteria were:
1) less than 23 weeks’ gestation;
2) admission to NICU more than 12 hours after
delivery; 3) presence of a lethal congenital
malformation; 4) death within the first 12 hours
of life.
The general characteristics of infants such
as gender, type of birth and Apgar scores of
first and fifth minutes, were extracted from
the infants’ cases and recorded in data
collection forms. The parameters of CRIB-II
were measured and recorded in data forms as
follows: Gestational age was calculated using
Ballard table or based on the first day of the
last menstrual period (LMP). In cases where
LMP was not known, gestational age was assessed
using obstetric ultrasonography. The infants
were weighed at the moment of admission with
digital scale of ±20 precision based
on gram unit. The infants’ body temperature
was measured axillary at the moment of admission
in NICU using digital thermometer with a sensitivity
of 0.1° C. Capillary blood gas analysis
was performed in all infants. Infants’
sex was determined through observing phenotype
of genitalia.
After measuring mentioned parameters, CRIB-II
score (range 0-27) (5) was calculated for each
infant and the prediction rate of it concerning
infants’ outcome was found based on CRIB-II.
The studied infants were followed up at 3 months
of age and their outcome (dying or staying alive)
was recorded in a data collection form. The
data were analyzed using SPSS software and to
determine the relationship between measured
parameters Spearman correlation was used. A
logistic model was used to analyze the prediction
of mortality using the CRIB II score on admission.
In all tests P<0.05 was considered as significant.
In
general,
272
neonates
were
investigated
in
this
study
and151
neonates
(52.9%)
and
121
neonates
(47.1%)
were
boys
and
girls,
respectively.
In
this
study,
160
neonates
(58.82%)
died
during
hospitalization
and
112
neonates
(41.18%)
survived
during
hospitalization
and
left
the
hospital.
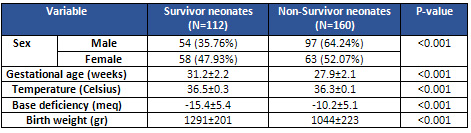
Gestational
age,
mean
body
temperature
and
mean
of
base
deficiency
(based
on
the
analysis
of
arterial
blood
gases)
in
survivor
neonates
were
less
than
non-survivor
neonates
and
these
differences
were
statistically
significant
(Table
1).
Table
1:
Evaluated
variables
in
CRIB
II
score
in
survivor
and
non-survivor
neonates
The
mean
of
CRIB
II
scores
for
non-survivor
neonates
and
survivors
was
9.7±3.1
and
6.1±2.7
respectively.
Statistical
analysis
showed
that
the
mean
of
CRIB
II
score
in
non-survivor
neonates
was
much
more
than
survivor
neonates
significantly
(PV<0.001).
The
mean
of
hospitalization
time
for
non-survivor
neonates
(5.1±4.5)
was
shorter
than
hospitalization
time
for
survivor
neonates
(15±9.8);
and
this
difference
was
statistically
significant
(PV<0.001).
In
survey
for
specificity
and
sensitivity
of
CRIB
II
score
in
mortality
prediction
of
premature
neonates
with
birth
weight
lower
than
1500
gr,
it
was
observed
that
almost
83%
(CI=74-91)
of
neonatal
mortalities
can
be
predicted.
In
the
present
study,
we
compared
risk
factors
of
neonatal
mortality
according
to
gestational
age
less
than
30
weeks,
body
temperature
less
than
36.5
centigrade,
Base
deficiency
less
than
-10,
birth
weight
less
than
1200
gr,
hospitalization
time
shorter
than
9
days
and
CRIB
II
score
more
or
equal
with
10
in
survivor
and
non-survivor
neonates.
The
results
showed
that
46%
of
non-survivor
neonates
and
9%
of
survivor
neonates
have
gestational
age
less
than
30
weeks
and
there
was
a
marked
difference
between
the
two
groups
(PV<0.001).
Also,
other
variants
were
significantly
much
better
in
survivor
neonates
than
non-survivor
neonates,
and
these
differences
were
statistically
significant
(PV<0.001).
In
our
investigations,
it
was
observed
that
CRIB
II
score
has
a
high
value
in
prediction
of
premature
neonates’
mortality
with
birth
weight
lower
than
1500
g,
in
a
way
that,
CRIB
II
score
could
predict
83%
of
mortality
cases
in
premature
neonates
that
shows
a
high
value
of
this
index.
Measurement
of
this
index
is
very
easy
and
fast
because
all
applied
variables
are
of
routine
investigations
of
low
weight
neonates;
also
these
variants
are
not
affected
by
human
errors.
Since
prediction
of
neonatal
mortality
with
very
low
birth
weight
(less
than
1500
gr)
reveals
an
outstanding
impact
on
medical
interventions,
in
different
studies,
and
various
indexed
were
studied
(5-9).
Felice
et
al
(2005)
studied
147
neonates
with
birth
weight
less
than
1500
gr
or
gestational
age
less
than
31
weeks.
They
evaluated
CRIB,
CRIB
II,
birth
age
and
birth
weight
for
prediction
of
neonatal
mortality;
according
to
AUC,
these
indexes
could
predict
mortality
between
86%
(birth
age)
to
92%
(CRIB).
The
researchers
did
not
observe
any
difference
between
investigated
indexes
in
prediction
of
neonatal
mortality
(10).
As
it
was
mentioned
previously,
in
our
study
all
indexes
were
valuable
in
prediction
of
neonatal
mortality.
Although
in
previous
studies
and
our
investigation,
CRIB
II
declared
higher
values
in
comparison
with
other
indexes
like
birth
age
and
birth
weight,
there
are
some
studies
that
have
evaluated
CRIB
II
as
less
predictive,
and
other
indexes
though
showed
there
was
no
significant
difference.
In
Baumer
et
al’s
study,
between
1991
to
2006,
1485
premature
neonates
were
studied.
In
this
investigation
based
on
AUC,
CRIB
82%,
birth
weight
74%,
birth
age
71%
and
CRIB
II
69%
could
predict
mortality
cases.
Although
there
was
no
statistically
significant
difference
between
the
indexes,
CRIB
II
has
lower
value
compared
to
other
indexes.
Asthere
is
no
clear
reason
for
these
observations,
researchers
believe
in
the
need
for
further
studies
(11).
Low
birth
weight
and
low
gestational
age
are
two
main
causes
of
numerous
disorders
in
these
neonates;
also
these
two
are
the
main
reason
for
mortality
in
infancy
and
the
first
year
after
birth
(12).
Disease
severity
of
the
neonate
at
hospitalization
time
and
some
laboratory
findings
like
Base
deficiency
rate
are
associated
with
the
prognosis
of
the
neonates.
Application
of
CRIB
as
a
simple
way
for
evaluation
of
illness
severity
during
hospitalization
that
can
estimate
the
relative
risk
of
neonatal
mortality
(13,
14).
In
a
survey
to
evaluate
the
CRIB
II
value
for
prediction
of
mortality
rate
of
premature
neonates
in
comparison
with
birth
weight
and
gestational
age,
97
neonates
were
investigated.
The
area
under
the
ROC
diagram
was
almost
equal
for
birth
weight,
gestational
age
and
CRIB
II.
The
result
of
this
research
showed
that
the
predictive
value
of
CRIB
II
score
in
prediction
of
mortality
rate
in
premature
neonates
is
not
more
than
birth
weight
and
gestational
age
(15).
Mortality
rate
of
premature
neonates
is
evaluable
by
CRIB
II.
In
an
investigation
to
compare
the
ability
of
CRIB,
CRIB
II,
birth
weight
and
gestational
age
in
prediction
of
premature
mortality,
1,485
neonates
were
studied.
The
area
under
the
AUC
graph
was
82%
for
CRIB,
74%
for
birth
weight,
71%
for
gestational
age,
and
69%
for
CRIB
II.
The
results
of
this
investigation
showed
that
CRIB
II
does
not
have
any
priority
over
birth
weight,
gestational
age
and
CRIB
in
determination
of
mortality
rate
of
premature
neonates
(16).
In
an
investigation
to
assess
the
ability
of
CRIB
in
determination
of
long-time
prognosis
of
neural
development
in
premature
neonates,
455
neonates
were
studied.
386
neonates
(89%)
survived
until
clearance
from
hospital
and
352
neonates
(91%)
were
investigated
mentally
when
they
were
1
year
old.
There
were
76
neonates
(22%)
with
a
major
neural
disorder.
Higher
CRIB
score
was
assigned
with
major
neural
disorder
(17).
In
addition,
in
another
investigation,
neonates
with
13
CRIB
II
score
or
more
at
first
hour
after
birth
had
major
developmental
disorders
(18).
In
another
study
which
was
conducted
in
Gorgan
university
of
medical
sciences,
in
order
to
evaluate
the
prognostic
power
of
CRIB
score
in
prediction
of
the
consequence
of
premature
VLBW
neonates,
46
neonates
with
gestational
age
less
than
37
weeks
and
birth
weight
lower
than
1500
gr
were
assayed.
Mortality
rate
in
this
research
was
37%
and
the
most
prevalent
reason
of
death
was
respiratory
failure.
The
mean
of
birth
weight,
gestational
age
and
the
mean
of
CRIB
score
in
the
group
of
survivor
neonates
and
non-survivor
neonates
was
1201,
934
gr
and
30
and
28
weeks,
and
3.76
and
11.47
respectively
(19).
In
our
investigation,
CRIB
II
scoring
system
was
used
to
determine
the
mortality
risk
in
neonates
with
birth
weight
less
than
1500
gr.
The
powerful
point
of
the
present
study
was
that
all
mentioned
variables
in
this
study
are
measured
routinely
in
all
neonates
with
birth
weight
less
than
1500
gr,
and
we
did
not
need
any
further
interventions.
Considering
this
point,
that
neonatal
state
at
first
hours
after
birth
is
related
to
midwifery
and
obstetric
issues
of
mother
and
problems
of
the
neonate,
the
measurement
of
these
variants
at
first
hours
after
birth
can
be
valuable
in
prediction
of
mortality
and
also
higher
score
in
CRIB
II
shows
higher
risk
of
mortality
for
neonate.
About
the
birth
weight
variant
in
prediction
of
neonatal
mortality,
it
should
be
said
that,
although
for
a
long
time
it
has
been
used
as
an
index
in
determination
of
neonatal
mortality,
numerous
studies
have
shown
that
prognosis
of
neonates
with
equal
weights
in
NICU
of
different
hospitals
are
different
and
that
can
be
related
to
the
applied
equipment
in
these
units,
proportion
of
nurses
to
patients
and
other
factors.
Limitations
of
the
Study
The
main
limitation
of
our
study
was
clearance
of
the
neonates
with
personal
satisfaction
of
the
parents
before
conduction
of
the
study
and
this
issue
was
solved
by
substitution
of
other
neonates.
According
to
our
findings
in
this
study,
CRIB
II
has
a
higher
value
in
mortality
prediction
of
the
neonates
with
birth
weight
lower
than
1500
gr
in
a
way
that,
it
could
predict
83%
of
mortalities
in
premature
neonates
with
birth
weight
lower
than
1500
gr
and
this
shows
the
high
value
of
this
index.
Since
the
prediction
of
neonatal
mortality
in
VLBW
neonates
(less
than
1500
gr)
has
a
high
value
in
medical
interventions,
CRIB
II
score
is
a
trustable
tool
in
neonatal
mortality
prediction
and
their
classification
is
to
make
priority
for
medical
interventions
especially
in
absence
of
medical
facilities.
1.
Waldemar
A.
Prematurity
and
Intrauterine
Growth
Restriction.
Robert
M
Kliegman,
Stanton.
Nelson
textbook
of
pediatrics.
19th
ed.
Philadelphia:
Saunders;
2011;
555-558.
2.
Basu
S,
Rathore
P,
Bhatia
BD.
Predictors
of
mortality
in
very
low
birth
weight
neonates
in
India.
Singapore
Med
J
2008;
49(7):556-60.
3.
Kliegman
Stanton
RM.
Nelson
textbook
of
pediatrics.
19th
ed.
Philadelphia:
Saunders;
2011
4.
Horbar
JD,
Gould
JB.
Evaluating
and
improving
the
quality
of
neonatal
care
in
neonatal
perinatal
medicine.
Fanaroff
AA,
Martin
RJ.
Disease
of
the
fetus
and
infant
.9th
ed.
Philadelphia:
Elsevier
Mosby;
2011;
56-75.
5.
Brito
AS,
Matsuo
T,
Gonzalez
MR,
de
Carvalho
AB,
Ferrari
LS.
CRIB
score,
birth
weight
and
gestational
age
in
neonatal
mortality
risk
evaluation.
Rev
Saude
Publica
2003;
37(5):
597-602.
6.
Gagliardi
L,
Cavazza
A,
Brunelli
A,
Battaglioli
M,
Merazzi
D,
Tandoi
F,
et
al.
Assessing
mortality
risk
in
very
low
birth
weight
infants:
a
comparison
of
CRIB,
CRIB-II,
and
SNAPPE-II.
Arch
Dis
Child
Fetal
Neonatal
Ed
2004;
89(5):
F
419-422.
7.
Rastogi
PK,
Sreenivas
V,
Kumar
N.
Validation
of
CRIB-II
for
prediction
of
mortality
in
premature
neonates.
Indian
Pediatr
2010;
47:
145-147.
8.
Marete
IK,
Wasunna
AO,
Otieno
PA.
Clinical
risk
index
for
neonates
(CRIB)
II
score
as
a
predictor
of
neonatal
mortality
among
low
birth
weight
neonates
at
Kenyatta
National
Hospital.
East
Afr
Med
J
2011;
88(1):
18-23.
9.
Guzmán
Cabañas
JM,
Párraga
Quiles
MJ,
del
Prado
N,
Ruíz
MD,
García
Del
Río
M,
Benito
Zaballo
F,
et
al.
Usefulness
of
Clinical
Risk
Index
for
Neonates
based
on
birth
weight
in
predicting
hospital
death
and
severe
intra-ventricular
hemorrhage
in
the
SEN
1500
Spanish
neonatal
network.
An
Pediatr
(Barc)
2009;
71(2):
117-127.
10.
De
Felice
C,
Del
Vecchio
A,
Latini
G.
Evaluating
illness
severity
for
very
low
birth
weight
infants:
CRIB
or
CRIB-II?
J
Matern
Fetal
Neonatal
Med
2005;
17(4):
257-260.
11.
Baumer
JH,
Wright
D,
Mill
T.
Illness
severity
measured
by
CRIB
score:
a
product
of
changes
in
perinatal
care?
Arch
Dis
Child
Fetal
Neonatal
Ed
1997;
77(3):
F211-
215.
12.
Vakrilova
V.
Scoring
systems
for
assessing
illness
severity
and
predicting
outcome
in
very
low
birth
weight
infants.
Akush
Ginekol
(Sofiia)
2011;
50(1):
37-41.
13.
Vakrilova
L,
Emilova
Z,
Sluncheva
B.
Using
the
CRIB
as
an
early
prognostic
index
for
very
low
birth
weight
infants,
treated
in
neonatal
intensive
care
units.
Akush
Ginekol
(Sofiia)
2007;
46
Suppl
1:66-73.
14.
Prieto
CL,
Colomer
BF,
Sastre
JB.
Prognostic
factors
of
mortality
in
very
low
birth
weight
infants
with
neonatal
sepsis
of
nosocomial
origin.
Am
J
Perinatol
2013;
30(5):
353-358.
15.
Khanna
R,
Taneja
V,Singh
S.
The
clinical
risk
index
of
neonates
(CRIB)
score
in
India.
Indian
J
Pediatr.
2002;
69(11):
957-960.
16.
Buhrer
C,
Metze
B,
Obladen
M.
CRIB,
CRIB-II,
birth
weight
or
gestational
age
to
assess
mortality
risk
in
very
low
birth
weight
infants?
Acta
Paediatr.
2008;
97(7):
899-903.
17.
Buhrer
C,
Grimmer
I,
Metze
B.
The
CRIB
(Clinical
Risk
Index
For
Babies)
score
and
neurodevelopmental
impairment
at
one
year
corrected
age
in
very
low
birth
weight
infants.
Intensive
Care
Med
2000;
26:
325-329.
18.
Lodha
A1,
Sauvé
R,
Chen
S,
Tang
S,
Christianson
H.
Clinical
Risk
Index
for
Babies
score
for
the
prediction
of
neurodevelopmental
outcomes
at
3
years
of
age
in
infants
of
very
low
birthweight.
Dev
Med
Child
Neurol.
2009;51(11):895-900.
19.
Fouladinejad
M,
Behnampour
N,
Pashaei
Zanjani
A,
Gharib
MH,
Akbari
Kamrani
M.
The
evaluation
of
predicting
mortality
risk
of
premature
infants
with
very
low
birthweght
by
CRIB
Score.
J
Gorgan
Uni
Med
Sci.
2009;10(4):40-43.
(In
Persian)
|
|
.................................................................................................................

|
| |
|
