|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
|
|
|
........................................................
In Memoriam
Professor
Orhan Ekrem Müftüoglu
|
........................................................
Original
Contribution / Clinical Investigation
|
|
Cholelithiasis
and cholecystectomy may lower the low density
lipoprotein cholesterol in plasma
DOI: 10.5742/MEWFM.2017.93010
[pdf
version]
Mehmet Rami Helvaci, Mursel Davarci, Orhan Veli
Ozkan, Ersan Semerci, Abdulrazak Abyad, Lesley
Pocock
Serum
and follicular fluid vitamin D and follicular
response among infertile women undergoing ICSI
DOI: 10.5742/MEWFM.2017.93011
[pdf
version]
Sedighe Esmaeilzadeh, Maryam Aliasgharpour,
Parvaneh Mirabi, Azita Ghanbarpour
Maede Fasihian
Studying
the relation of quality of work life with socio-economic
status and general health among the employees
working in Students Welfare Fund of Ministry
of Health and Medical Education in 2016
DOI: 10.5742/MEWFM.2017.93012
[pdf
version]
Saeed Reza Azami, Nasrin Shaarbafchizadeh, Soheil
Mokhtari, Ali Maher
On the Effect
of Cognitive Behavioural Counseling on Sexual
Satisfaction of Mothers with Autistic Children:
A Randomized Clinical Trial
DOI:
[pdf version]
Leila Arbil, Mitra Kolivand, Farzaneh Golboni,
Effat MerghatiKhoei, Mansour Rezaei
Pre-operative
sublingual misoprostol and intra-operative blood
loss during total abdominal hysterectomy: a
randomized single-blinded controlled clinical
trial
DOI: 10.5742/MEWFM.2017.93013
[pdf
version]
Taravat Fakheri, Tayebe Noori
Investigating
the Effect of Endotracheal Tube Cuff Pressure
on Sore Throat, Hoarseness and Cough in Patients
with Coronary Artery Bypass Surgery
DOI: 10.5742/MEWFM.2017.93014
[pdf
version]
Ali Akbar Vaezi, Mohammad Hassan Mondegari Bamakan
Comparing
the Self-Esteem and Resiliency between Blind
and Sighted Children and Adolescents in Kermanshah
City
DOI: 10.5742/MEWFM.2017.93015
[pdf
version]
Saeedeh Bakhshi, Nafiseh Montazeri , Babak Nazari,
Arash Ziapour, Hashem Barahooyi,
Fatemeh Dehghan
|
........................................................
Population
and Community Studies
|
|
Frequency
of Uric Acid Levels, Symptomatic and Asymptomatic
Hyperuricemia among the Pakistani Population
DOI: 10.5742/MEWFM.2017.93016
[pdf
version]
Waris Qidwai, Masood Jawaid
Determinants
of Tooth Brushing among Primary School Students
DOI: 10.5742/MEWFM.2017.93017
[pdf
version]
Mohammad Mahboubi, Mohammad Ismail Motlagh,
Mehdi Mirzaei-Alavijeh, Farzad Jalilian, Hassan
Gharibnavaz,
Mohammad Fattahi
Depression
in patients suffering from gender dysphoria:
The hospitalized patients of Legal Medicine
Center in Southwest of Iran
DOI: 10.5742/MEWFM.2017.93018
[pdf
version]
Zahra Gorjian, Mohammad Zarenezhad, Mohhamad
Mahboubi, Saeid Gholamzadeh,
Nahid Mahmoodi
An epidemiological
study of suicide attempts and to determine the
correlation between attempted suicide causes
and demographic characteristics of people in
Kermanshah Province during a year
DOI: 10.5742/MEWFM.2017.93019
[pdf
version]
Hamid Reza Shetabi, Samira Rostami, Mohsen Mohammadi,
Mahsa Cheleii, Lida Saedi, Saba Amiri Nasab,
Shirin Zardui GolAnbari
The
effectiveness of life skills training on happiness,
mental health, and marital satisfaction in wives
of Iran-Iraq war veterans
DOI: 10.5742/MEWFM.2017.93038
[pdf
version]
Kamal Solati
The
Role of Self-Compassion Factors in Predicting
the Marital Satisfaction of Staff at Kermanshah
University of Medical Sciences
DOI:10.5742/MEWFM.2017.93020
[pdf
version]
Parisa Janjani, Lida Haghnazari, Farahnaz Keshavarzi,
Alireza Rai
Mediating
role of irrational beliefs in the relationship
between the quality of family communication
and marital satisfaction
DOI:10.5742/MEWFM.2017.93021
[pdf
version]
Parisa Janjani, Khodamorad Momeni, Alireza Rai,
Mohammad Reza Saidi
|
........................................................
Review Article
........................................................
International Health
Affairs
........................................................
Education
and Training
........................................................
Clinical
Research and Methods
|
|
Adaptive
LASSO Logistic Regression applied on gene expression
of prostate cancer
DOI: 10.5742/MEWFM.2017.93028
[pdf version]
Amir Hossein Hashemian, Maryam Ghobadi Asl,
Soodeh Shahsavari, Mansour Rezaei,
Hadi Raeisi Shahraki
The
prevalence of brain and neck injuries in patients
with maxillofacial fractures in teaching hospitals
of Rasht in 2016
DOI: 10.5742/MEWFM.2017.93029
[pdf
version]
Seyed Mohammad Talebzadeh, Ali Khalighi Sigaroudi,
Babak Alijani, Safa Motevasseli,
Saied Dashtyari, Mahsa Shariati, Zeinab Davoudmanesh
Cultural
competency: a concept analysis in TUMS (Tehran
University of Medical Science) DOI:
10.5742/MEWFM.2017.93030
[pdf version]
Foruzan Khatamidoost, Mandana Shirazy, Hamid
Khankeh, Nemat Allah Musapour
Majid Sadeghi, Kamran Soltani Arabshahi
The
Effect of Proprioceptive Neuromuscular Facilitation
(PNF) on Activities of Daily Living of client
with Cerebrovascular accident
DOI: 10.5742/MEWFM.2017.93031
[pdf
version]
Najafi Doulatabad Shahla, Afrasiabifar Ardashir,
Parandvar Yaghoub
Evaluation
of the ratio of T helper 17 and T regulatory
cells in patients with chronic idiopathic urticaria
DOI: 10.5742/MEWFM.2017.93032
[pdf
version]
Hossein Shahriari, Farahzad Jabbari, Seyyed
Abdolrahim Rezaee, Houshang Rafatpanah
Majid Jafari, Reza Farid Hosseini, Majid Asadi-Samani
|
........................................................
Model
and System of Primary Care
........................................................
Case
Series and Case Reports
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| September 2017
- Volume 15, Issue 7 |
|
|
The prevalence of brain
and neck injuries in patients with maxillofacial
fractures in teaching hospitals of Rasht in
2016
Seyed
Mohammad Talebzadeh (1)
Ali Khalighi Sigaroudi (2)
Babak Alijani (3)
Safa Motevasseli (4)
Saied Dashtyari (5)
Mahsa Shariati (6)
Zeinab Davoudmanesh (7)
(1) Resident, Department of Oral and Maxillofacial
Surgery, Dental Sciences Research Center, Faculty
of Dentistry, Guilan University of Medical Sciences,
Rasht, Iran
(2) Assistant Professor, Department of Oral
and Maxillofacial Surgery, Dental Sciences Research
Center, Faculty of Dentistry, Guilan University
of Medical Sciences, Rasht, Iran
(3) Assistant Professor, Department of Neurosurgery,
Faculty of Medicine, University of Medical Sciences,
Rasht, Iran
(4) Assistant Professor, Department of Oral
and Maxillofacial Surgery, Dental Sciences Research
Center, Faculty of Dentistry, Guilan University
of Medical Sciences, Rasht, Iran
(5) Assistant Professor, Department of Oral
and Maxillofacial Surgery, Dental Sciences Research
Center, Faculty of Dentistry, Guilan University
of Medical Sciences, Rasht, Iran
(6) Department of Orthodontics and Dentofacial
Orthopaedics, Tehran University of Medical Sciences,
Shariati Hospital, Tehran, Iranbranch, Tehran,
Iran, Islamic republic of Iran
(7) Dentist, Member of craniomaxillofacial Research
Center, Tehran University of medical sciences,
Tehran, Iran, Member of craniomaxillofacial
research center, Islamic Azad University, Tehran,
Iran
Correspondence:
Zeinab Davoudmanesh
Dentist, Member of craniomaxillofacial Research
Center,
Tehran University of medical sciences,
Tehran, Iran
|
Abstract
This study aimed
to determine the prevalence of brain and
neck injuries in patients with maxillofacial
fractures in teaching hospitals of the
city of Rasht in 2016. This is an analytical
retrospective study. Some 361 patients
of the training centers of Rasht which
had been diagnosed with maxillofacial
fractures entered the study, 286 of which
were male and 75 were female. Information
collected through questionnaires and records
of the patients who admitted to emergency
department of Poursina and Velayat hospitals
with maxillofacial fractures. The patients
were examined to see whether they have
brain and cervical spine injuries. The
diagnosis of the fracture and brain and
neck injuries had been separately written
by the related doctors on the records
of the patients based on clinical examination
and Plain radiography and CT scans. After
data collection, the results were analyzed.
The resultsshowed that 61 percent of the
fractures were due to accidents. Among
the most common spine damage, (77 percent)
was related to bone fractures. The highest
frequency of brain damage was related
to Extradural Hematoma by 23.65 percent.
Results of the treatments also showed
that 76% of the patients partially recovered.
Key words: brain
injuries, neck injuries, maxillofacial
fractures
|
In the last 20 years, facial bone fractures
have been common injuries in patients admitted
to emergency departments of hospitals(1) so
that nearly one third of injured patients have
some kind of trauma in this area. Prevalence
and causes of maxillofacial injuries vary in
different countries. In developing countries,
the most prevalent cause of maxillofacial injuries
is car accidents (1). Statistics indicate an
increase in death toll of traffic accidents
in Iran in recent years (2). In developed countries
such as America, damages resulting from trauma
(especially vehicle crashes) is the seventh
leading cause of death (3). Several studies
conducted around the world show that young pedestrians
(children and teenagers) and the elderly are
two high risk groups in traffic accidents. Motorcycle
riders are another high risk group in traffic
accidents (2, 3). Mokerjy et al (4) demonstrated
in their study that from 714 patients with fractures,
traffic accident was the cause of 88 percent
of the fractures. Shazia (5) also indicated
that in all cases of maxillofacial fractures,
the cause was traffic accidents.
The face is one of the most vulnerable parts
of the body. At the time of an accident, due
to the proximity of vital organs such as the
brain and its sheaths, the spinal cord, the
cervical spinal cord and eyes and also due to
physiological problems (controlling airway and
breathing), cosmetic and psychological factors,
can lead to serious complications for patients
(3).
The most common facial bones fracture is in
the bones of the lower face (Mandible) and the
less common one is in the upper face. The middle
part of the face is in the intermediate state
between Mandible and Frontal (6). The upper
and middle part fractures are more severe than
lower part fractures and if left untreated,
will cause a lot of deformity (6). Maxillary
bone forms most of the middle part. The bone
plays a major role in forming the look and the
beauty of the person. It also has a major role
in the formation of lower lip and orbital bone.
Maxillary fractures are of different types.
The most common types of these fractures include
fractures of Le Fort I, II, III, and fractures
of alveolar maxilla and sagittal maxilla (6
and 7). Maxilla fractures are caused by a direct
hit from the front or from the side. Today,
most of these fractures are caused by traffic
accidents. Face and jaw fractures are accompanied
by complications such as nasal airway obstruction,
the problem in the cranial cavity and Dura rupture,
damage to the anterior part of the brain, dental
occlusion disorder, obstruction of Lacrimal
system, abnormalities in appearance, blindness,
anophthalmia, diplopia, and loss of sensation
in the territory of Infra orbital nerve (8).
Several studies also show that fractures in
the facial area have led to brain and spinal
cord problems. The study of Grant et al (9),
which was conducted in the US, determined that
brain damage in people with facial fractures
was generally at 67 percent. A study conducted
by Farevash et al (18) revealed that among his
population the fracture of Le Fort II was the
most prevalent. As for associated fractures,
zygomatic fractures were 62%, mandible fracture
25%, nasoethmoidal fracture 9% and skull base
fracture was 4%. Hugh et al (10) in a study
showed that the incidence of brain damage associated
with facial fractures is estimated to be 17.5
percent. Kraos et al (11) showed that facial
fractures are very effective on brain injuries.
In many patients with facial fractures, there
is likely not enough attention paid to brain
and cervical spine damage and also given the
importance of facial fractures and the fairly
conflicting results of previous studies (12),
we decided to investigate the relationship between
maxillofacial fractures and brain and neck damage.
In
this
descriptive-analytical
and
retrospective
study
which
was
conducted
as
a
cross-sectional
study
in
2016,
361
people
who
were
admitted
to
the
training
centers
in
Rasht
with
maxillofacial
fractures
entered
the
study.
286
of
them
were
male
and
75
were
female.
The
majority
of
the
participants
in
this
study
(129
people)
were
between
the
ages
of
21
and
30.
Information
was
collected
through
questionnaires
and
patients’
records
who
were
admitted
to
the
emergency
department
of
Poursina
and
Velayat
hospitals
with
maxillofacial
fractures.
The
patients
were
examined
to
see
whether
they
have
brain
and
cervical
spine
injuries.
The
diagnosis
of
the
fracture
and
brain
and
neck
injuries
had
been
separately
written
by
the
related
doctors
on
the
records
of
the
patients,
based
on
clinical
examination
and
Plain
radiography
and
CT
scans.
Cases
that
were
incomplete
for
various
reasons
were
omitted.
Data
was
collected
by
questionnaires
and
was
entered
into
SPSS
software
for
analysis.
To
describe
the
data,
descriptive
tests
were
used.
The
results
of
the
data
collection
showed
that
traffic
accidents
were
the
most
prevalent
cause
of
the
fractures
in
the
patients
of
this
study
(61
percent).
Data
also
showed
that
the
pattern
of
maxillofacial
fractures
was
as
follows:
mandibular
fractures
(51%),
maxillary
fractures
(4%),
zygomatic
fractures
(6%),
frontal
fractures
(10%),
nose
fractures
(10%)
and
compound
fractures
(8
percent).
So,
the
mandible
was
the
most
common
area
of
fractures
in
patients.
In
all
fractured
areas,
frequency
in
men
was
more
than
in
women.
As
for
the
fracture
pattern,
there
was
a
significant
difference
between
patients
(p=0/0001)
as
well
as
between
the
two
sexes
(men
and
women).
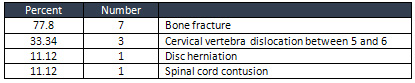
In
Table
1,
the
results
of
the
most
common
injuries
of
the
cervical
spine
in
patients
are
presented.
The
most
common
cervical
spine
injuries
were
as
follows
bone
fractures
(77.8
percent),
cervical
vertebrae
dislocation
(33.34
percent),
disc
herniation
(11.12
percent)
and
spinal
cord
contusion
(11.12
percent).
Considering
the
types
of
cervical
spine
injuries,
there
was
a
statistically
significant
difference
between
patients
(p=0/0001).
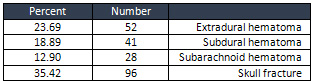
In
Table
2,
the
most
common
brain
damage
in
patients
is
presented.
Among
the
different
types
of
skull
fractures,
fractures
of
the
frontal
bone
were
of
the
highest
frequency
among
patients
(37.5
percent)
which
were
followed
by
Ethmoid
bone
fractures
(29.32
percent),
orbital
roof
(16.67
percent)
and
the
sphenoid
bone
fractures
(13.54
percent)
(p
=0/041).
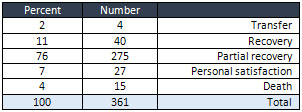
Table
3
presents
the
results
of
treatment
(recovery,
death,
etc.)
in
the
studied
patients.
The
majority
of
patients
(76%)
left
the
hospital
with
partial
recovery.
11
percent
improved
and
7
percent
were
discharged
with
personal
satisfaction.
4%
of
the
patients
died
and
2%
transferred
to
other
medical
centers.
Table
1:
The
most
common
cervical
spine
injuries
 Table
2:
The
most
common
brain
injuries
Table
2:
The
most
common
brain
injuries
 Table
3:
Results
of
treatment
(recovery,
death,
etc)
in
the
patients
Table
3:
Results
of
treatment
(recovery,
death,
etc)
in
the
patients
| DISCUSSION
AND
CONCLUSION
|
As
discussed,
trauma
is
one
of
the
leading
causes
of
death
in
the
communities.
Maxillofacial
fractures
are
one
of
the
main
problems
of
trauma
patients.
Facial
Fractures
are
likely
to
be
associated
with
complications
such
as
brain
and
spinal
cord
damage.
With
this
description,
this
study
aimed
to
examine
the
prevalence
of
brain
and
cervical
damage
in
patients
with
maxillofacial
fractures.
The
first
finding
of
the
present
study
was
that
the
most
important
cause
of
maxillofacial
fractures
is
car
accidents
with
61
percent.
In
most
studies
in
Iran
(13,
14,
and
15),
car
accidents
have
also
been
considered
as
the
most
common
cause
of
fractures.
Also,
similar
results
were
obtained
from
studies
of
Patrocinio
et
al
(16),
Adebayo
et
al
(17),
Klenk
and
Kovacs
(18).
In
a
review
article
by
Oikarinen
et
al
(19),
etiologic
differences
of
maxillofacial
fractures
in
Kuwait,
Canada
and
Finland
were
compared.
The
researchers
found
that
traffic
accidents
were
the
cause
of
55
percent
of
fractures
in
Kuwait,
33
percent
of
fractures
in
Finland
and
7%
in
Canada.
These
results
are
consistent
with
information
obtained
by
the
Kuwaiti
researchers
who
showed
that
Eastern
countries
do
not
observe
the
traffic
rules.
However,
the
percentage
of
injuries
caused
by
conflict
in
Kuwait
is
(12%),
Finland
(37%)
and
Canada
(54
%).
The
second
finding
of
the
present
study
is
that
the
mandible
(51%)
was
the
most
common
site
of
fractures
in
patients.
This
finding
was
consistent
with
the
findings
of
Akrami
Abargouei
et
al
(20)
Kamoliga
et
al
(21),
Maliska
et
al
(22),
Blasilirov
and
Pasry
(23),
Karkaovik
et
al
(24),
and
it
is
inconsistent
with
research
of
Dongas
and
Hall
(25).
Akrami
Abargouei
et
al
(20)
reported
that
in
patients
with
maxillofacial
fractures,
the
most
common
site
of
involvement
is
the
nasal
bone
(67.4%)
followed
by
mandible
(18.7
percent).
In
this
study,
the
most
common
site
of
involvement
in
the
mandibular
condyle
(31.47
percent)
and
the
body
of
the
mandible
(26.73
percent).
Dongas
and
Hull
in
their
study
reached
the
conclusion
that
the
fracture
of
the
middle
third
of
the
face
is
the
most
common
site
of
involvement.
The
third
finding
of
the
study
is
that
the
most
common
injury
of
the
cervical
spine
of
the
subjects
of
this
study
was
bone
fracture
(77.8%)
and
cervical
vertebrae
dislocation
(33/34
%).
The
findings
of
the
study
were
similar
to
those
of
Mokerji
et
al
(4).
In
his
study,
fracture
and
dislocation
of
the
cervical
vertebrae
was
a
total
of
63
percent
and
disc
herniation
and
spinal
cord
contusion
were
37%
among
the
patients.
The
researchers
also
noted
that
70
percent
of
the
injuries
of
the
cervical
spine
have
occurred
at
levels
of
C1
/
C2
or
C6
/
C7.
The
fourth
finding
of
this
study
is
that
among
various
types
of
skull
fractures,
frontal
bone
fracture
had
the
highest
frequency
in
samples
of
this
study
(37.5
percent).
This
is
consistent
with
the
findings
of
Yadave
et
al
(26).
In
the
study
of
Yadave
et
al
(26),
extradural
hematoma,
subdural
hematoma
and
subarachnoid
hematoma
in
patients
with
maxillofacial
fractures
were
also
reported
22,
17
and
14
percent,
respectively.
In
this
study,
frontal
fracture,
sphenoid
fracture
and
orbital
roof
fracture
were
21,
11
and
14
percent
respectively.
Although
this
study
has
limitations
including
lack
of
generalizability
of
the
results,
according
to
the
findings
of
the
study,
it
can
be
summarized
that
the
maxillofacial
fractures
are
accompanied
by
brain
and
spinal
cord
injuries
and
this
fact
was
confirmed
in
the
subjects
of
this
study.
Traffic
accidents
were
the
main
cause
of
maxillofacial
fractures
in
this
study.
World
Health
Organization’s
guidelines
on
the
main
factors
in
preventing
accidents
are
as
follows:
the
use
of
safety
belts,
helmets,
seats
for
children,
not
using
mobile
phones
while
driving
and
improving
the
safety
of
roads.
Better
design
of
roads
and
highways,
training
courses
for
drivers
and
implementation
of
more
serious
measures
should
also
be
considered.
Despite
the
preventive
laws
for
mandatory
use
of
safety
devices,
indices
of
cooperation
in
the
society
affect
the
performance
of
these
safety
solutions.
1.
Dongas
P,
Hall
GM.
Mandibular
fracture
patterns
in
Tasmania,
Australia.
Aust
Dent
J.
2002;47(2):131-7.
2.
Naghavi
M.
Mortality
in
18
provinces
of
Iran
in
1380.
Health
Deputy.
Tehran:
Iran
Ministry
of
Health
and
medical
Education
2003:
171-73.
3.
Hoyt
DB,
Coimbra
R,
Potenza
B.
Management
of
acute
trauma.
In:
Townsend
CM,
Beauchamp
RD,
Evers
BM,
Mattox
K,
eds.
Sabiston
Textbook
of
Surgery.
WB
Saunders,
17th
ed
2004:483.
4.
Mukherjee
S,
Abhinav
K,
Revington
PJ.
A
review
of
cervical
spine
injury
associated
with
maxillofacial
trauma
at
a
UK
tertiary
referral
centre
Ann
R
Coll
Surg
Engl
2015;
97:
66–72.
5.
Shazia
Y.
Facial
trauma
among
patients
with
head
injuries.
Journal
of
IMAB
-
Annual
Proceeding
(Scientific
Papers)
2014,
vol.
20,
issue
6.
6.Lindqvist
C,
Lizuka
T.
Facial
trauma
as
a
result
of
work-related
accidents.
Suom
Hammaslaakarilehti
1990;
37:
872-81.
7.Manson
PN.
Facial
injuries.
In:
McCarthy
JG,
editor.
Plastic
Surgery.
Philadelphia,
PA:
WB
Saunders
Co;
1990.
p.
867-1141.
8.Kwon
PH,
Laskin
DM.
Clinician’s
Manual
of
Oral
and
Maxillofacial
Surgery.
3rd
ed.
Chicago,
IL:
Quintessence;
2000.
9.
Lalani
Z,
Bonanthaya
KM.
Cervical
spine
injury
in
maxillofacial
trauma.
Br
J
Oral
Maxillofac
Surg
1997;
35:
243-5.
9.Grant
AL,
Ranger
A,
Young
GB,
Yazdani
A.:
Incidence
of
major
and
minor
brain
injuries
in
facial
fractures:
J
Craniofac
Surg.
2012
Sep;23(5):1324-8.
10.
Haug
RH,
Savage
JD,
Likavec
MJ,
Conforti
PJ
A
review
of
100
closed
head
injuries
associated
with
facial
fractures.
J
Oral
Maxillofac
Surg.
1992
Mar;50(3):218-2.
11.
Kraus
JF,
Rice
TM,
Peek-Asa
C,
McArthur
DL.
Facial
trauma
and
the
risk
of
intracranial
injury
in
motorcycle
riders.
Ann
Emerg
Med.
2003
Jan;41(1):18-26.
12.
Keenan
HT,
Brundage
SI,
Thompson
DC,
Maier
RV,
Rivara
FP:
Does
the
face
protect
the
brain?
A-case-
control
study
of
traumatic
brain
injury
and
facial
fractures.
Arch
Surg.
1999;
134:14-17.
13.
Ansari
MH.
Maxillofacial
fractures
in
Hamedan
province,
Iran:
a
retrospective
study
(1987-2001).
J
Craniomaxillofac
Surg
2004;
32(1):28-34.
14.
Motamedi
MH.
An
assessment
of
maxillofacial
fractures:
a
5-year
study
of
237
patients.
J
Oral
Maxillofac
Surg
2003;61(1):61-4.
15.
Faryabi
J.
Epidemiological
survey
of
maxillofacial
injuries
in
patients
admitted
to
Bahonar
hospital
of
Kerman
City
during
1996-2002.
J
Dent
Sch
2004;
21(4):544-51.
16.
Patrocínio
LG,
Patrocínio
JA,
Borba
BH,
Bonatti
Bde
S,
Pinto
LF,
Vieira
JV,
Costa
JM.
Mandibular
fracture:
analysis
of
293
patients
treated
in
the
Hospital
of
Clinics,
Federal
University
of
Uberlândia.
Braz
J
Otorhinolaryngol
2005;71(5):560-5.
17.
Adebayo
ET,
Ajike
OS,
Adekeye
EO.
Analysis
of
the
pattern
of
maxillofacial
fractures
in
Kaduna,
Nigeria.
Br
J
Oral
Maxillofac
Surg
2003;41(6):396-400.
18.
Klenk
G,
Kovacs
A.
Etiology
and
patterns
of
facial
fractures
in
the
United
Arab
Emirates.
J
Cranio
Maxillofac
Surg
2003;
14(1):
78-84.
19.
Oikarinen
K,
Schutz
P,
Thalib
L,
Sándor
GK,
Clokie
C,
Meisami
T,
et
al.
Differences
in
the
etiology
of
mandibular
fractures
in
Kuwait,
Canada,
and
Finland.
Dent
Traumatol
2004;20(5):241–5.
20.
Akrami
Sh,
Navab
Azam
A,
Akaberi
F.
Epidemiologic
investigation
of
maxillofacial
fractures
in
admitted
patients
in
Yazd
trauma
centers
(2005-2011).Yazd
Journal
of
dental
research.
2014,2(1),46-60.
21.
Kamulegeya
A,
Lakor
F,
Kabenge
K.
Oral
maxillofacial
fractures
seen
at
a
Ugandan
tertiary
hospital:
a
sixmonth
prospective
study.
Clinics
(Sao
Paulo).
2009;64(9):843-8.
22.
Maliska
MC,
Lima
Júnior
SM,
Gil
JN.
Analysis
of
185
maxillofacial
fractures
in
the
state
of
Santa
Catarina,
Brazil.
Braz
Oral
Res
2009;23(3):268-74.
23.
Brasileiro
BF,
Passeri
LA.
Epidemiological
analysis
of
maxillofacial
fractures
in
Brazil:
a
Five-year
prospective
study.
Oral
Surg
Oral
Med
Oral
Pathol
Oral
Radiol
Endod
2006;102(1):28-34.
24.
Chrcanovic
BR,
Freire-Maia
B,
Souza
LN,
Arajo
VO,
Abreu
MH.
Facial
fractures:
a
1-year
retrospective
study
in
a
hospital
in
Belo
Horizonte.
Braz
Oral
Res
2004;18(4):322-8.
25.
Dongas
P,
Hall
GM.
Mandibular
fracture
patterns
in
Tasmania,
Australia.
Aust
Dent
J.
2002;
47(2):131-7.
26.
Yadav
SK,
Mandal
BK,
Karn
A,
Sah
AK.
Maxillofacial
trauma
with
head
injuries
at
a
tertiary
care
hospital
in
Chitwan,
Nepal:
clinical,
medico-legal,
and
critical
care
concerns
Turk
J
Med
Sci
2012;
42
(Sup.2):
1505-1512.
|
|
.................................................................................................................

|
| |
|
