|
Studying the relation
of quality of work life with socio-economic
status and general health among the employees
working in Students Welfare Fund of Ministry
of Health and Medical Education in 2016
Saeed
Reza Azami (1)
Nasrin Shaarbafchizadeh (2)
Soheil Mokhtari (3)
Ali Maher (4)
(1) Ph.D candidate in Health Services Management,
Department of Health Services
Management ,Azad University -North Tehran Branch.Tehran,Iran
(2) Assistant Professor in Health Services Management,
Health Management and Economics
Research Center, Isfahan University of Medical
Sciences, Isfahan
(3) B.Sc. Student, Health Management and Economics
Research Center, Iran University of
Medical Sciences, Tehran, Iran.
(4) Ph.D.Assistant Professor, Department of
Health Services Management, Tehran North Branch,
Islamic Azad University, Tehran, Iran
Correspondence:
Ali Maher, Ph.D.Assistant Professor,
Department of Health Services Management,
Tehran North Branch,Islamic Azad University,
Tehran, Iran
|
Abstract
Introduction:
The importance of socio-economic variables
such as level of literacy, income, and
occupational
status and their impact on the physical
and psychological well-being of the people
is clear for experts and policymakers.
In much research, the root of increase
in life expectancy and improvement in
other indexes of health is considered
to not only progress medicine, but also
improve socio-economic indexes. Thus,
the present study aims to determine the
relation between socio-economic status
and general health and the consequences
of disease on the quality of work life
of the employees working in Students Welfare
Fund of Ministry of Health and Medical
Education.
Methodology:
The present cross-sectional research
is of descriptive-analytical type, that
has been conducted in Students Welfare
Fund of Ministry of Health and Medical
Education in 2016, and the population
under study included all the 130 employees
working in the Students Welfare Fund.
The required data was collected by consensus
method and Quality of Work life (QWL)
questionnaire. This questionnaire was
based on Walton components and Socio-economic
Status (SES) questionnaire, and was designed
in order to evaluate socio-economic status,
and had 4 components. The data on general
health was collected by Goldberg and Hillier
28-Item General Health Questionnaire (GHQ-28)
(1979). Then, the collected data was recorded
by SPSS version 18 software and was analyzed
by common methods of descriptive-analytical
statistics.
Results: The results demonstrated
that the frequency of socio-economic status
of the employees under study were 73 persons
(57.9 percent) for low level, 45 persons
(35.7 percent) for moderate level, and
8 persons (6.3 percent) for high level,
and the frequency of the quality of work
life of the employees under study were
7 persons (5.6 percent) for low level,
40 persons (32.3 percent) for moderate
level, and 77 persons (62.1 percent) for
high level.
Conclusion:
Considering the importance of quality
of work life in socio-economic status,
it is proposed that the following measures
be taken into account: appropriateness
of salary to the economic factors like
inflation; demand and supply in fair and
adequate payment; paying more attention
to the physical conditions of workplace,
e.g. light, cooling and heating facilities
to prepare a secure and healthy workplace;
preparing some possibilities for the employees
so that they can further develop their
personal talents and have opportunities
for making progress in their specialized
field by encouraging creativity and innovation
that leads to the promotion of the organization;
and providing continuous security and
growth opportunities for the employees,
allowing them to do of their own free
will, and providing any information or
skill that they need in the workplace
to develop their human capabilities. In
the present study, there is a significant
relationship between the quality of work
life and general health and also socio-economic
status and general health, however, there
was no significant relationship between
quality of
work life and socio-economic status.
Key words:
Quality of Work life (QWL), socio-economic
status, general health, employees working
in Students Welfare Fund.
|
Nowadays organizations are considered as living
creatures with an identity that is independent
of their members (1), and by this new identity,
they can affect the behavior of their employees.
This personality and identity can be organizationally
healthy or ill (2). Miles introduced the notion
of “organizational health” in 1969.
In his view, organizational health refers to
the durability and persistence of an organization
in its environment and adaptability to it, and
also developing its own ability to be more adaptable
to it (3). Wrong choice, misuse of skills, and
lack of proper atmosphere to allow creativity
to flourish can endanger health and promotion
of the organization. When a position or office
is proposed for employees that is not commensurate
with their dignity, it can lead to disobedience,
absence from work, delays, and resignation.
In an organization, if communication at all
levels is not multilaterally and openly established,
and full confidence does not exist between different
parts, misunderstanding and disharmony will
be created. When goals are not clear, they become
vague, and as a result, the employees do not
make a concerted effort to achieve the goals
(4).
Recently the human factor has been considered
as the most important and sensitive organizational
element, and most of the new theories of organization
and management have referred to this sensitive
factor (5). One of the most important parameters
affecting the performance of human resources
is the role of individual health in improving
the economy of a country. Therefore, any kind
of planning or investment in human resources
that leads to protect and promote the health
of employees, can eventually lead to increased
efficiency and Return on Investment (ROI) (6).
Nowadays the notion of quality of work life
has turned into a major social issue all around
the world, while in the past the emphasis was
only on personal life. From the 1970s onward,
improving the employees’ quality of work
life has been considered as one of the most
important issues in many organizations, including
health care organizations (7). Due to the inevitability
of some of the stress factors in health care
organizations and the need to prevent psychological
stress effects, one of the duties of managers
in these organizations is taking some measures
and actions to improve the quality of work life,
and teaching coping techniques (8). Although
there is no formal definition of quality of
work life, however, Walton’s theory has
offered the most comprehensive components of
quality of work life plan (9). He has offered
the main components of quality of work life
in four dimensions that are as follows: meaningfulness
of work; organizational and social fit of work;
provocativeness, richness, and fruitfulness
of work; and security, developing skills, and
continuous learning in work (10).
Quality of work life programs deal with various
objective and subjective areas of employees’
issues. Quality of work life is a process by
which the organization’s members can participate
in making decisions that generally affect their
job and particularly their work environment;
in doing so, they can use open and appropriate
communication ways that have been designed for
this purpose. As a result, their work-related
stress will diminish and employees’ satisfaction
will increase. An organization that pays attention
to its employees’ quality of work life
will benefit from having competent workforce,
the signs of which are willingness to cooperate
with the management and improvement in the performance
of the workforce (11).
General health is a subset of the health system
and is defined as a set of important social
activities and measures that are based primarily
on prevention strategies (12). One of the characteristics
of a healthy organization is that the physical
and psychological health of the employees are
as important and interesting as production and
productivity for its managers (13). In recent
decades various studies have been conducted
on the relationship between work and stress
and its consequences for health care workers.
In these studies, some topics such as productivity,
occupational accidents, absenteeism, and increase
in physical and mental damage in various occupational
groups have been scrutinized (14). The profession
of the people is one of the main causes of stress
in their life. There is more stress in professions
in which human contact is important (15).
Socio-economic determinants of health such
as level of income, education, job, nutrition,
and social class are far more important in catching
diseases than the biological factors, and they
play an important role in human’s health
(16). In the social hierarchy, people take different
positions based on their occupational status
and level of education and income, and the position
of the people in this system is defined by their
socio-economic status. Although occupation and
level of income and education all determine
the position of an individual in the social
hierarchy, these factors are generally not separate
from each other, but they should be individually
studied in order to realize their role in health.
Level of education makes differences in terms
of having access to information and level of
expertise to take advantage of knowledge, while
occupation entails differences in having access
to scarce material goods. Occupational status
includes both of these aspects, and also includes
benefits of working in certain occupations such
as dignity, privilege, and technical and social
skills and power (17).
The present age organizations have a strategic
approach to human resources and consider it
as a smart and valuable asset, and desire to
further improve the quality of life and job
satisfaction of their employees (18). Workplace
health and psychological health are created
by improving quality of life indexes, and it
is necessary to pay attention to this issue
in all organizations in order to prevent job
burnout and low efficiency. Measuring the understanding
and sense of people about their own health in
order to assess the status quo, investigating
the efficacy of health interventions and health
care, and implementing appropriate health services
are of crucial importance (19). Socio-economic
status is an important factor that affects the
possibility of taking advantage of medical services,
while the wealthy social groups, which in every
respect are better equipped than the disadvantaged
groups, can sooner and better convert their
need to demand, and hence, take more advantage
(20). A survey of 17,000 employees in England
showed that occupation rank itself plays a more
important role in health than some risk factors
combined, such as smoking and high blood pressure
and cholesterol. Since healthy human is the
axis of sustainable development, and also modern
societies call for providing a proper environment
for production and having the required speed
to achieve comprehensive development, it is
clearly the responsibility of health practitioners
and researchers to investigate and explain all
the social factors influencing health, and then
giving feedback to the policy-makers in the
form of scientific and practical information.
In this way, they can help a great deal toward
sustainable development (21).
The importance of socio-economic variables
such as level of education, income, and occupational
status, and their impact on physical and psychological
health of the people, is clear for health experts
and policy-makers. It has been suggested in
many studies that increase in life expectancy
and improvement in the other health indexes
are not merely because of medical progress,
but in many cases are due to the improvement
in the socio-economic indexes (22).
Global data shows that environment, socio-economic
status, housing, job security, access to health
facilities, and human behavior are all crucial
factors in securing or weakening health (23).
Research in many countries shows extensive inequalities
and differences in health conditions of various
socio-economic, racial, ethnic, and geographical
groups in society. This is indicative of the
crucial impact of various factors on health
that include reducing social exclusion, alleviating
educational shortcomings, reducing insecurity
and unemployment, and improving housing standards
(24).
Studies on the relationship between health
and socio-economic status of a population originally
started in England. Gradually this type of research
was of interest to researchers in other countries
and useful data was collected in this field,
all of which shows that individuals and families
who are in lower social groups, in comparison
to higher and richer social groups, experience
more and premature death, and diseases and defects
are more common in this group; this inequality
can be seen in all European countries, and is
an undeniable fact that needs more attention
(23). To this aim, this research has been conducted
to determine the relationship between socio-economic
status and general health, and show the consequences
of disease that affects the quality of work
life of Students Welfare Fund employees.
This study is of descriptive-analytical type
that has been conducted by cross-sectional method
in Students Welfare Fund in 2016, and the population
under study included all the 130 employees working
in Students Welfare Fund. The inclusion criterion
for the study was being an employee in Students
Welfare Fund, i.e. all the employees working
in the Fund and the employees working in Khazarabad
Complex in Sari. Quality of Work life (QWL)
questionnaire was used to collect the required
data. This questionnaire was based on Walton’s
components, including fair and adequate payment
(questions 1 to 5), safe and healthy working
environment (questions 6 to 8), providing growth
opportunities and continuous security (questions
9 to 11), having respect for the laws in the
organization (questions 12 to 17), social dependence
of work life (questions 18 to 20), the overall
atmosphere of life (questions 21 to 25), social
integrity and solidarity (questions 26 to 29),
and developing human capabilities (questions
30 to 32). This questionnaire has been conducted
by many researchers and contains 32 items, and
is based on a Likert scale from very low (1
point) to very high (5 points).
Walton showed the reliability coefficient of
the questionnaire to be 0.88 (25). Also in 2006
Rahimi reported the reliability coefficient
of the test to be 0.85 (1). Furthermore, in
this study, the Socio-economic Status (SES)
questionnaire is implemented, which takes four
components of income, economic class, education,
and housing into account, and generally consists
of 6 demographic questions and 5 key questions.
The criterion scaling of questions in this questionnaire
has 5 options and responses are graded on a
continuum, from very low (1) to very high (5).
Eslami et al. (26), by asking 12 sports experts,
has confirmed the face
and content validity of this questionnaire. Also
by applying Cronbach’s alpha test, the reliability
of the questionnaire was calculated as 0.83. General
health data were collected by Goldberg and Hillier
28-Item General Health Questionnaire (GHQ-28)
(1979). It has 4 subscales and each subscale contains
7 questions. These subscales include somatic symptoms,
anxiety and insomnia, social dysfunction and severe
depression. Of the 28 items of the questionnaire,
questions 1 to 7 are about somatic symptoms, questions
8 to 14 ask about anxiety and insomnia, questions
15 to 21 assess social dysfunction, and finally,
questions 22 to 28 are related to severe depression.
In standardization of GHQ-28 questionnaire
in Iran, Houman (1997) implemented Cronbach’s
alpha coefficient for the subscales to assess
the internal consistency of it, and reported
them to be 0.85, 0.87, 0.79, and 0.91, respectively.
For the overall score, that demonstrates general
health, he reported 0.85. Goldberg and Blackwell
(1972), by using a clinical interview checklist
for 200 surgery patients in England, and concluded
that more than 90% of the sample was correctly
classified by the questionnaire as sick or healthy.
Moreover, they reported the correlation coefficient
between the scores of GHQ-28 questionnaire and
the result of clinical evaluation of the results
to be 0.80. Also they reported sensitivity and
specificity as 0.84 and 0.82, respectively.
In order to assess the socio-economic status,
the Socio-economic Status (SES) Questionnaire
(Ghodratnama, 2013) was generally implemented.
This questionnaire contains 4 components, namely
income, economic class, education, and housing,
and in total contains six demographic questions
and 5 key questions. Criterion scaling in this
questionnaire consisted of five responses, and
the scoring method for each response was from
very low (1) to very high (5). Eslami et al.
(26), by asking 12 sports experts, has confirmed
the face and content validity of this questionnaire.
Also by applying Cronbach’s alpha test,
the reliability of the questionnaire was calculated
as 0.83 (28).
Thus, the collected data were recorded by SPSS
version 18 software and then underwent statistical
analysis. By using common methods in descriptive-analytical
statistics, the results were demonstrated in
the forms of tables, diagrams, etc.
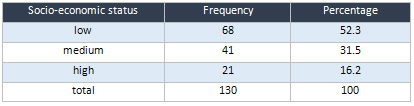
The
results
demonstrated
that
the
frequency
of
socio-economic
status
of
the
studied
employees
were
68
for
low
status
(52.3%),
41
for
medium
status
(31.5%),
and
21
for
high
status
(16.2%).
Table
1:
Socio-economic
Status
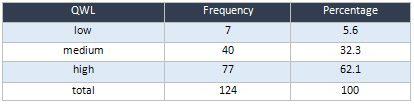
The
results
demonstrated
that
the
frequency
of
quality
of
work
life
of
studied
employees
were
7
for
low
status
(5.6%),
40
for
medium
status
(32.3%),
and
77
for
high
status
(62.1%).
Table
2:
Frequency
and
percentage
of
Quality
of
Work
Life
(QWL)
status
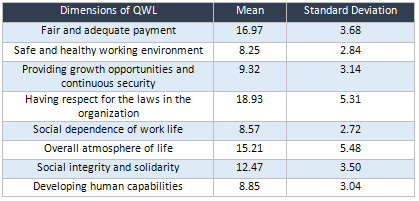
The
results
demonstrated
that
the
mean
and
standard
deviation
of
dimensions
of
quality
of
work
life
were
16.97
and
3.68
for
fair
and
adequate
payment,
8.25
and
2.84
for
safe
and
healthy
working
environment,
9.32
and
3.14
for
providing
growth
opportunities
and
continuous
security,
18.93
and
5.31
for
having
respect
for
the
laws
in
the
organization,
8.57
and
2.72
for
social
dependence
of
work
life,
15.21
and
5.48
for
the
overall
atmosphere
of
life,
12.47
and
3.50
for
social
integrity
and
solidarity,
and
8.85
and
3.04
for
developing
human
capabilities.
Table
3:
Status
of
QWL’s
dimensions
The
results
demonstrated
that
in
the
somatic
dimension
of
employee’s
general
health,
50
persons
were
at
very
low
level
(39.1%),
53
persons
were
at
slight
level
(41.1%),
18
persons
were
at
medium
level
(14.1%),
and
7
persons
were
at
severe
level
(5.5%).
In
anxiety
dimension,
41
persons
were
at
very
low
level
(32.8%),
49
persons
were
at
slight
level
(39.2%),
30
persons
at
medium
level
(24%),
and
5
persons
at
severe
level
(4%).
In
social
dimension,
33
persons
were
at
very
low
level
(25.8%),
77
persons
at
slight
level
(60.2%),
16
persons
at
medium
level
(12.5%),
and
2
persons
at
severe
level
(1.6%).
In
depression
dimension,
104
persons
were
at
very
low
level
(81.3%),
19
persons
at
slight
level
(14.8%),
4
persons
at
medium
level
(3.1%),
and
1
person
at
severe
level
(0.8%):
Click
here
for
Table
4:
Status
of
total
general
health
and
its
dimensions
The
results
of
the
test
demonstrate
that
among
the
employees
that
in
terms
of
socio-economic
status
were
at
a
low
level,
3
persons
(4.3%)
had
low
quality
of
life.
Of
those
employees
that
had
a
medium
socio-economic
status,
2
persons
(4.7%)
had
low
quality
of
life.
Also,
1
person
(12.5%)
among
the
employees
with
high
socio-economic
status,
had
medium
quality
of
work
life.
The
results
of
Chi-squared
test
show
that
there
is
no
significant
relationship
between
socio-economic
status
and
quality
of
work
life
(p=0.086).
Click
here
for
Table
5:
Quality
of
work
life
status
in
terms
of
socio-economic
status
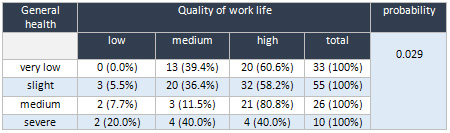
The
results
of
the
test
show
that
among
the
employees
with
a
very
low
level
of
general
health,
20
persons
(60.6%)
had
high
quality
of
work
life,
while
among
the
employees
with
slight
general
health,
32
persons
(58.2%)
had
high
quality
of
work
life.
Also
among
the
employees
with
a
medium
general
health,
21
persons
(80.8%)
had
high
quality
of
work
life,
and
among
the
employees
with
severe
general
health,
4
persons
(40.0%)
had
high
quality
of
life.
The
results
of
Fisher
test
show
that
there
is
a
significant
relationship
between
general
health
and
quality
of
work
life
(p=0.029).
Table
6:
General
health
in
terms
of
quality
of
work
life
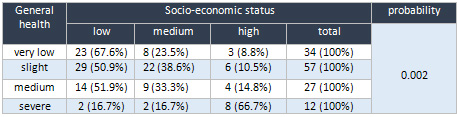
The
results
of
the
test
show
that
among
the
employees
with
a
very
low
level
of
general
health,
23
persons
(67.6%)
had
a
low
socio-economic
status,
and
among
the
employees
with
a
slight
level
of
general
health,
29
persons
(50.9%)
had
a
low
socio-economic
status.
Also
among
the
employees
with
a
medium
level
of
general
health,
14
persons
(51.9%)
had
a
low
socio-economic
status,
and
among
the
employees
with
a
severe
general
health,
2
persons
(16.7%)
had
a
low
socio-economic
status.
The
results
of
Fisher
test
show
that
there
is
a
significant
relationship
between
general
health
and
socio-economic
status
(p=0.002).
Table
7:
General
health
in
terms
of
socio-economic
status
| DISCUSSION
AND
CONCLUSION |
The
purpose
of
this
study
was
to
investigate
the
relationship
of
quality
work
life
with
socio-economic
status
and
general
health
among
the
employees
working
in
Students
Welfare
Fund
of
Ministry
of
Health
and
Medical
Education.
According
to
the
descriptive
results
of
the
present
study,
most
of
the
employees
(almost
52%)
had
a
low
level
of
socio-economic
status.
The
results
of
the
study
show
that
the
frequency
of
socio-economic
status
of
the
employees
under
study
were
179
(53.3%)
for
low
level,
109
(35.5%)
for
medium
level,
and
199
(6.2%)
for
high
level.
Also
the
frequency
of
employees’
quality
of
work
life
were
10
(3.3%)
for
low
level,
108
(35.6
%)
for
medium
level,
and
185
(61.1%)
for
high
level,
while
most
of
them
(almost
62%)
had
a
high
quality
of
work
life.
As
mentioned
before,
in
order
to
study
the
quality
of
work
life
of
the
employees,
these
components
were
taken
into
account:
fair
and
adequate
payment,
safe
and
healthy
working
environment,
providing
growth
opportunities
and
continuous
security,
having
respect
for
the
laws
in
the
organization,
social
dependence
of
work
life,
overall
atmosphere
of
life,
social
integrity
and
solidarity,
and
developing
human
capabilities.
Among
these
factors,
having
respect
for
the
laws
in
the
organization
and
fair
and
adequate
payment
respectively
had
the
highest
average
in
the
quality
of
work
life
of
the
employees.
General
health,
was
the
other
objective
of
this
study;
most
of
the
employees
working
in
the
Students
Welfare
Fund
(almost
38.4%)
were
at
slight
level.
Of
the
studied
dimensions
of
general
health,
most
of
the
employees
reported
their
status
to
be
at
slight
level
in
somatic,
anxiety,
and
social
dimensions,
and
only
a
few
of
them
reported
to
be
at
severe
level
in
these
dimensions.
However,
in
depression
dimension,
most
of
the
studied
employees
(81.3%)
reported
to
be
at
a
very
low
level,
and
only
a
few
of
them
(almost
1
percent)
reported
severe
depression.
The
results
of
this
study
are
in
line
with
the
study
of
Dargahi
et
al.,
in
which
the
general
health
status
of
the
executive
managers
was
investigated,
and
the
highest
and
the
lowest
average
scores
and
frequency
percentages
related
to
social
and
depression
dimensions,
respectively.
Furthermore,
the
managers
in
this
study
were
at
an
appropriate
status
in
other
dimensions
of
general
health
(somatic
and
psychological),
and
this
is
in
line
with
the
results
of
the
present
study.
The
other
issue
relates
to
the
analytical
findings.
The
results
of
the
test
shows
that
the
employees
in
terms
of
general
health
were
at
a
very
low
level;
23
persons
(67.6%)
had
a
low
socio-economic
level,
and
among
the
employees
who
were
at
a
slight
level
of
general
health,
29
persons
(50.9%)
had
a
low
socio-economic
level.
Among
the
employees
who
were
at
a
medium
level
of
general
health,
14
persons
(51.9%)
had
low
socio-economic
level,
and
of
the
employees
who
were
at
a
severe
level
of
general
health,
2
persons
(16.7%)
had
low
socio-economic
status.
The
results
of
the
Fisher
test
show
that
there
is
a
significant
relationship
between
general
health
and
socio-economic
status
(p=0.002).
In
addition
to
studying
the
relationship
between
each
of
the
variables
of
general
health
and
socio-economic
status
with
the
quality
of
work
life
of
employees
in
this
study,
there
is
a
significant
relationship
between
quality
of
work
life
and
general
health,
and
also
between
socio-economic
status
and
general
health,
but
there
is
no
significant
relationship
between
quality
of
work
life
and
socio-economic
status.
Hence,
the
relation
between
each
one
of
the
dimensions
of
general
health
with
socio-economic
status
was
investigated,
and
the
results
of
the
Fisher
test
showed
that
there
is
no
significant
relationship
between
dimensions
of
general
health
(somatic,
anxiety,
social,
dimension)
and
socio-economic
status.
Considering
the
findings
of
this
study,
and
in
order
to
promote
the
socio-economic
status
of
the
employees
working
in
the
Students
Welfare
Fund
of
Ministry
of
Health
and
Medical
Education,
it
is
suggested
that
the
authorities
pay
especial
attention
to
these
suggestions:
fair
and
adequate
payment,
providing
growth
opportunities
and
continuous
security,
having
respect
for
the
laws
in
the
organization,
and
developing
human
capabilities.
Furthermore,
implementing
some
policies
in
order
to
reduce
depression
and
anxiety
and
increase
social
function
of
the
employees
can
enhance
their
quality
of
work
life.
1.
Seyed
javadian
R.The
principle
of
organization
and
Management.
Tehran:
Negah
Danesh;
2005.
[Persian].
2.
Saatchi
M.
Work
psychology:
Application
of
psychology
at
work,
organization
and
management.
Tehran:
Virayesh;
2004.
[Persian].
3.
Jahed
H.
organizational
health.
Tadbir
training
scientific
monthly
2005;
(159):
10-16.
[Persian].
4.
Daft
R.
Organization
Theory
&
design.
(Translate
by:
Parsayan
A,
A’arabi
M).
6Th
ed.
Tehran:
cultural
Research
Bureau;
2004.
[Persian].
5.
Botshekan,
Mohammad
Hashem.
Promoting
management
capacity
and
motivation
for
employees
working
in
institutions
and
organizations.
Management
and
Planning
Organization
of
Iran.
1995.
6.
Spinaci
S,
Korat
L,
Keravel
V.
Tough
choices
investment
in
health
for
development.
7.
Khaghanizadr
M,
Ebadi
A,
Siratinayer
M,
Rahmani
M.
[The
Study
of
Relationship
between
job
stress
and
quality
of
work
life
of
nursesin
military
hospital].
Mil
Med
2008;
10
(3);
175-84.Persian.
8.
McVicar
A.
Workplace
stress
in
nursing:
a
literature
review.
J
Adv
Nurs.2003;
44(6):633-42.
9.
Organization
WH.
TheWorld
health
report:
2001:
Mental
health:
new
understanding,
new
hope.2001.
10.
Conklin
MH,
Desselle
SP.
Snapshot
of
pharmacy
faculty
quality
of
work
life
and
productivity.
Journal
of
Pharmacy
Teaching.2007:14(1):53-77.
11.
Ballou
B,
Norman
H,
Goodwin
NH.
Quality
of
work
life.
Strategic
Finance.2007:89(4):40-51.
12.
Davari
SA.
Health
and
its
determinants.
Tehran,
contemporary
works,
2007:
25.
13.
Saatchi
M.
Applied
Psychology
for
Managers
in
homes,
schools
and
organizations.
1nd
ed.
Tehran:editing,
1995:
5-
51.
14.
Stellman
JM,
McCann
M,
Warshaw
L,
et
al.
Encyclopaedia
of
occupational
health
and
safety.
4th
ed.
Geneva:
International
Labour
Office.
34.2-34.28.
1998.
15.
Bahribinabaj
N,
Moghimian
M,
Attarbashi
M,
Gharche
M.
Inverstigating
the
relationship
between
job
burnout
and
mental
health
in
nursing
and
midwifery
professions.
Ofogh-e
Danesh.
Journal
of
Gonabad
University
of
Medical
Sciences.
2003,
Vol.
9,
Spring
and
Summer.
1:
99-104.
16.
Motlaq
M,
Oliaee
Manesh
A,
Beheshtian
M.
Health
and
its
social
determinants.
2nd
ed.Tehran:
Moafaq
Press;
2007.
42
[In
Persian].
17.
Lahelma
E,
Kivela
K,
Roos
E,
Tuominen
T,
Dahl
E,
Diderichsen
F,et
al.
Analysing
changes
of
health
inequalities
in
the
Nordic
welfare
states.
Social
Science
of
Medicine
2002;
55:
609-25.
18.
Bazaz
Jazayeri
SA,
Pardakhtchi
MH.
[Developing
a
model
for
the
assessment
of
quality
of
work
life
in
organizations].
Iranian
Journal
of
Management
Sciences
2007;
2(5):123-51.
19.
Nejat
S,
Montazeri
A,
Holakoie
K,Mohamad
K,Majdzadeh
SR.
Quality
of
Life
of
Tehran’s
population
by
Whoqol-Bref
questionnaire
in
2005.Hakim
2007;
10(3):
1-8.
20.
Spinaci
S,
Korat
L,
Keravel
V.
Tough
choices
investment
in
health
for
development.
Ttranslated
by:
Poorreza
A.
1st
ed.
Tehran:
University
Of
Medical
Science
Prees;
2008.
38-9
[InPersian].
21.
Marmot
M,
Wilkinson
R.
Social
determinants
of
health.
Translated
by:
Montazeri
A.
1st
ed.
Publication
of
Jahad;
2008.
1-30.
22.
http://www.unicef.org/sowc08/profiles/child_survival.php.
Last
accessed
at
2011-03-14.
23.
Alemi,
Ali
Akbar.
Poverty
and
its
influences
on
health,
experinces
and
Mistakes
of
the
West.
Tahghighat
and
Amoozesh
Company
Publications.
Fall
2001.
24.
Davoudi,
Saeed.
Health
and
its
Determinants.
Ministry
of
Health
and
Medical
Education,
Health
Department.
2007.
25.
Virme,
G.
(2001).
“Human
behaviour
;
improving
performance
at
work”.
New
York
:
Perntice-Hell,
inc.
26.
Eslami,
Ayoub.
Mahmoudi,
Ahmad.
Khabiri,
Mohammad.
Najafian
Razavi,
Seyed
Mehdi.
(2013).
The
role
of
Socio-economic
status
in
motivating
the
people
to
participate
in
public
and
recreational
sports.
Journal
of
Applied
research
in
sport
management,
2
(3),
89-104
27.
Fahti
Ashtiani,
Ali.
Psychological
tests
-
personality
and
mental
health
evaluation.
Besat
Publications.
2009.
28.Sa’atchi,
Mahmoud.
Kamkari,
Kambiz.
Askarian,
Mahnaz.
Psychological
tests.
Virayesh
Publications.
2010.
|

