|
Depression in patients
suffering from gender dysphoria: The hospitalized
patients of Legal Medicine Center in Southwest
of Iran
Zahra
Gorjian
(1)
Mohammad Zarenezhad
(2)
Mohhamad Mahboubi
(3)
Saeid Gholamzadeh
(4)
Nahid Mahmoudi (5)
(1) MSc, Faculty member of Department of Nursing,
Abadan School of Medical Sciences, Abadan, Iran.
(2) MD, PhD Candidate, Legal Medicine Research
Center, Legal Medicine Organization, Tehran,
Iran.
(3) PhD in Health Services management, faculty
member of department of health, Abadan School
of Medical Sciences, Abadan, Iran.
(4) MD, General practitioner, Legal Medicine
Research Center, Legal Medicine Organization,
Tehran, Iran.
(5) Student Research Committee, Abadan School
of Medical SciencesA badan, Iran.
Correspondence:
Nahid Mahmoudi,
Student Research Committee, Abadan School of
Medical Sciences,
Abadan, Iran
|
Abstract
Background and Aims: Sexual
identity is a kind of cognitive phenomenon
which shows an individual as a male or
female. The main problem regarding this
issue is the violation of gender identity
through which the patients are to change
their behaviors based on their gender
identity. In this case, the patients are
not understood by their friends and family.
Consequently, they are overlooked by other
people and will be disappointed. This
issue may lead them to be hopeless and
lose their confidence and finally become
depressed. This research was to compare
the patients who became depressed before
and after surgery of gender dysphoria
in the southwest of Iran, Fars Province.
Method:
This study is a survey research which
has studied all the population with gender
dysphoria who were referred to Legal Medicine
Center in Fars province in the southwest
of Iran. The research sample included
the 66 patients who were selected based
on convenience sampling method. Data were
collected through Becks’ (1961) Depression
Questionnaire. Data were analyzed through
Mann Whitney U test, Pearson correlation
analysis, and convenience sampling method
through SPSS’ version 21 at the significance
level (p<0.05).
Results: Findings
showed that the participants were between
18 and 36 years old and mainly had nongovernmental
jobs (i.e., free job) about (60.7%). Their
educational level was mainly below the
diploma (i.e., about 55%). The amount
of depression was in potential status
(51.97±7.39) and in actual status
was (51.35±6.91) regarding a severe
condition. The Mann Whitney analysis showed
that there was not a significant difference
between before and after surgery of the
patients with gender dysphoria (p = 0.67).
There was a correlation between age and
depression (r= .389) after the surgery.
However, there was not a correlation between
depression and other demographic variables
(i.e., age, Gender, Occupation, Educational
level) in both groups (p<0.05)
Conclusion:
In conclusion, results showed that gender
dysphoria patients face many challenges
like isolation, family conflict, finding
jobs or partner after surgery which are
due to Iranian cultural, social and religious
beliefs. They become isolated and depressed
and they have the same situation like
before the treatment and surgery.
Key words:
Gender dysphoria, depression, sex reassignment
surgery
|
Sex is an everlasting phenomenon which is with
human beings to the end of life. In social processes,
the individuals learn how to behave and feel,
based on their sex and become a member of the
society. They learn how to behave based on social
expectations. Being successful in the process,
the individuals can shape their gender identity
and adapted it to society (Ceglie, 2000). Sociologists
believe that gender is a phenomenon which is
unique and it is affected by social and cultural
learning (Correll, 2001); however, it is violated
when it istreated prejudicially. In other words,
the individuals may physically have a specific
sex but they do not feel they belong to that
sex spiritually or physically. These people
may behave or feel like the opposite sex. Indeed,
this bisexual situation may affect their psychological
condition and weaken their appropriate performance
(Ceglie, 2000).
Sexual identity is a cognitive phenomenon which
shows that an individual is male or female (Saddock,
2009). In fact, individuals have a kind of sexual
identity which shapes their beliefs, attitudes
and behaviors in a stereotyped fashion (Tavassoli,
2014). Freud believes that the sexual malbehaviors
are rooted in people’s childhood which
is experienced by children’s Oedipal Triangle.
It means, the children experience the behaviors
of their parents and they try to adapt to the
same situation (Utnam, 2003).
The patients of gender dysphoria are the people
whose appearance is different to what they view
as their actual sex. They need to change their
appearance to their gender identity (Veale,
2010). Some of these patients are the people
with male appearance but have female gender
identity (Male to Female). The other group may
be the opposite. They are female in appearance
but their gender identity is male (Female to
Male). This phenomenon is seen among males (Sohn,
2007).
The social pressure on patients with gender
dysphoria is too severe since they cannot manage
their behaviors in a cooperative way with their
counter parts (Matsomoto, 2009). The main form
of this problem is called appealing to sex reassignment
surgery based on IV DSM that shows 1 person
per 30,000 males and 1 person per 100,000 females
wish to change their sex (APA, 2000). Therefore,
these patients face many sexual problems since
they have some limitations (i. e., physical,
sexual and job condition) which cause conflicts
with their family and society. They also face
isolation and ignorance imposed by their family
and society. In fact, they suffer from affective
ties which make them isolated. This can cause
loneliness, lack of self-confidence, fear of
judgment and feeling unattractive (Gomez, 2012).
Regarding, Iranian culture, the patients of
gender dysphoria were not recognized as real
patients but they were known as criminal persons
and they cannot be accepted by many people.
This creates stress and psychological problems
for these people (Rahimi, 2016).
One of the main problems with gender dysphoria
could be depression and suicide which are due
to other people’s negligence and ignorance.
People also blame the individuals with this
problem and do not see them as patients (Cook,
2004). Gorin- Lazard (2012) studied these people
and concluded that these people have a shorter
life than others since they experience depression
which shortens their life. The research on 298
women with gender dysphoria in Boston, the USA
in 2012-2015 showed that 35.4 percent were severely
depressed and 14.7 present had a suicide history
(Reisner, 2016).
The treatment of gender dysphoria could be
a combination of surgery and taking hormone
medicine which changes the physical appearance.
This can assist in helping the patients to adapt.
The permission for sex reassignment surgery
can be issued 12 months after experiencing the
real new life and 6 months after taking hormone
treatment (Lothstein, 1980).
Family affective support is the main factor
for successful sex reassignment surgery (Besharat,
2012). They hope that these patients can regain
their self- confidence and reduce their depression
and anxiety to have a better life. Although
there are some reports which has noted that
sex reassignment surgery has positive effects
on the patients’ lives, their sexual activities
may cause complicated sexual problems since
they activate their sexual activities more than
before the surgery. This shows that these changes
are just limited to their physical appearance
(Anisworth, 2010; Gorin, 2012; Life, 1993; Pakic,
1996). In this case, some patients after the
surgery remain weakened and sensitive (De Cuypere,
2006). In a study, it was seen that 30 percent
of males and 20 percent of females who had undergone
surgery never experienced satisfaction (Asgari,
2007).
Therefore, the present study investigated the
patients before and after surgery in Fars Province,
Southwest of Iran. This surgery costs much for
the patients who have to pass a problematic
process to receive permission. Thus the aim
is to know whether this treatment can free them
from depression.
This study was designed based on a survey research
on the cases of gender dysphoria in the legal
medicine Organization in Fars province. They
received permission and were classified into
two groups:
A) The patients who were referred to
Fars legal medicine organization or the psychotherapy
clinics received some advice and they were recognized
as candidates for the surgery based on (DSM-IV).
Diagnostic and statistical manual of mental
disorders- 4th edition.
B) The patients who had an operation
two or ten years ago based on the recognition
of the Fars psychiatrics of Legal Medicine Organization
(LMO) International classification of disease
– 10th revision (ICD-10, 1988, and DSM-IV,
1994).
The research population included 80 patients
who were referred to LMO or the psychiatrics
offices in Fars province. Following the Morgan
table, the research sample included 66 patients
who were selected through non-random convenience
sampling method. They were selected among those
patients who accepted to participate in the
research process. Thus all patients included
males and females who were not equal in one
group and 38 patients in the second group were
selected.
The criterion for selection was the recognition
based on DSM-IV-TR. The other criterion included
the patients’ cooperation, their profile,
the reports of their surgery, psychological
status, and some ethical issues like patients’
privacy. Sampling process took four months.
The explanation was given to all patients and
they were required to fill in the questionnaires.
In this process, their privacy, ethical values
and cooperation were followed based on the Helsinki
treaty (Javaheri, 2006). Finally, after completing
the questionnaires, the researchers collected
the data. The inventory was Beck’s (1961)
Depression questionnaire which included demographic
information. Beck Depression Inventory (BDI-II)
includes 21 multiple choice items and each item
holds the scores from zero (mental health) to
3 (severe depression) and every respondent receives
a score from zero to 64. The inventory items
include depression factors of sadness, pessimism,
lack of enjoyment, lack of self-confidence,
sensitivity, lack of concentration, etc. The
scores between 0-4 is low level and it means
there is no depression. From 5 to 7 there is
a minimum level of depression. The scores from
8 to 15 is medium depression and the score above
16 shows the highest level of depression.
Beck and colleagues reported the internal consistency
of this instrument as (r=.73) to (r=.92) with
the average of (r=.86) and Alpha level (a=.86)
for the patients and (r=.81) for healthy people.
This reliability has been reported in some studies
(e.g., Beck, 1984, 2000; Alto, 2012; Shafer,
2006; Nuevo, 2009).
Data were analyzed through descriptive statistics
(i. e., Frequency, mean and standard deviation)
and inferential statistics (i. e. Pearson correlation
coefficient, and Mann U Whitney) through Statistical
Package for Social Sciences (SPSS), version
21. In the present study Beck’s questionnaire
was given to 21 participants and its Cronbach
alpha was (0.733) at the significant level (p<0.05).
Sixty
six
participants
participated
in
the
present
study.
28
participants
received
surgery
and
38
did
not
receive
an
operation.
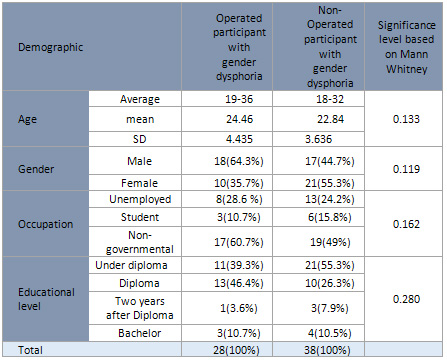
The
mean
of
age
among
the
before
surgery
group
was
22.84
±3.636
and
among
the
after
surgery
group
it
was
24.46±4.435.
Totally,
31
females
and
35
males
participated
in
the
present
study.
In
the
operated
group
the
highest
frequency
included
13
(46.4%)
participants
with
diploma
at
the
educational
level
and
17
(60.7%)
participants
who
had
non-governmental
jobs.
The
range
of
their
age
was
from
19
to
36
years
old.
21
non-operated
highest
frequency
participants
who
held
diploma
included
21
(55.3%)
participants
(55.3%)
and
19
(49%)
participants
had
non-
governmental
jobs.
Their
age
ranged
from
18
to
32
years
old
(see
Table
1).
Table
1:
Demographic
variable
(i.e.,
age,
gender
and
educational
level)
among
operated
and
non-operated
participants
In
the
present
the
amount
of
depression
showed
no
significant
difference
between
the
two
groups
and
the
results
showed
that
the
patients
with
gender
dysphoria
in
both
operated
and
non-operated
group
were
suffering
from
severe
depression
(p=0.691).
The
results
are
shown
in
Tables
2
and
3.
Table
2.
Descriptive
statistics
of
depression
among
operated
and
non-
operated
participants

Table
3.
The
Mean
of
depression
in
operated
and
non-operated
participants

Moreover,
the
correlation
between
the
amount
of
depression
with
the
demographic
variable
like
age,
gender,
job,
and
educational
level
in
both
groups
was
analyzed.
In
the
operated
group,
there
was
a
significant
correlation
between
depression
and
age
(r=.389)
but
the
correlation
between
depression
and
other
demographic
variables
was
not
significantly
seen
(p<0.05).
Table
4
shows
the
results.
Table
4.
The
correlation
coefficient
of
depression
with
demographic
variable

Since
the
data
were
not
normally
distributed,
the
analysis
of
Mann
Whitney
U
test
was
used
to
compare
the
difference
of
depression
in
the
two
groups.
Table
2
shows
that
there
is
not
a
significant
difference
between
the
two
groups’
depression
(P=0.691)
although
the
difference
exists,
it
does
not
reach
significant
level
(p<0.05).
To
calculate
the
correlation
between
depression
and
age,
Pearson
correlation
was
used.
Table
4
shows
that
the
correlation
of
depression
and
age
is
significant
(0.389)
in
the
operated
group
at
the
significant
level
(p<0.05).
The
eta
square
was
used
to
measure
the
correlation
of
depression
and
other
demographic
variables.
Results
show
that
there
is
not
a
significant
correlation
between
depression
and
demographic
variables
like
gender,
occupation
and
educational
level.
|
DISCUSSION
AND
CONCLUSION
|
The
findings
of
this
study
showed
that
the
difference
between
the
two
groups’
depression
was
not
significant.
The
amount
of
depression
was
severe
in
both
groups.
This
may
be
explained
in
terms
of
the
cost
that
the
patients
have
to
pay
for
the
operation
and
the
processes
which
are
very
difficult
(Michel,
2002).
These
patients
face
the
opposition
of
their
families.
They
are
often
jobless
or
work
in
non-governmental
institutes.
Thus
they
cannot
afford
the
operation
cost.
This
may
make
them
depressed.
These
patients
are
dealing
with
physical,
mental
and
social
problems
and
look
at
the
operation
as
the
way
they
can
be
free
from
these
problems.
Sometimes,
the
presence
of
their
names
in
the
operation
list
can
help
them
to
overcome
depression
(Michel,
2002).
The
results
of
the
present
study
are
in
line
with
Reisner
(2016)
who
studied
298
females
with
dysphoria
in
Boston,
US.
From
2012
to
2015.
The
results
showed
that
35.4%
of
them
had
severe
depression
and
14.7%
of
them
had
suicide
history.
The
results
are
also
matched
with
De
Cuyopere
(2006)
who
conducted
a
longitudinal
study
on
60
patients
with
gender
dysphoria
and
noted
that
they
faced
high
level
of
anxiety
and
depression.
Several
studies
(e.
g.
.,
Hepp,
2005),
reported
the
highest
correlation
between
gender
dysphoria
and
other
mental
disorders.
Campo
(2003)
in
a
study
reports
that
gender
dysphoria
is
correlated
to
personality
disorder
(79%)
and
ill-mannered
behavior
(20%).
Katz
and
colleagues
(1985)
studied
the
patients
who
were
suffering
from
gender
dysphoria.
They
found
that
the
children
with
gender
dysphoria
were
suffering
from
anxiety,
depression,
and
behavioral
affective
problems.
Some
of
these
patients
experienced
learning
problems
and
failure
in
schools.
Committing
suicide
was
also
seen
among
these
patients.
The
results
of
this
study,
however,
were
not
matched
with
several
studies
(i,
e.,
Cardoso,
2016).
For
example,
in
the
study,
conducted
by
Cardoso
(2016),
results
showed
that
47
patients
with
operation
(MTF)
showed
better
mental
health
in
social
and
psychological
relations
after
a
year
of
operation.
But
they
faced
physical
problems
and
self-independent
relations.
Farner
and
Cocust
found
that
the
patients
after
operation
overcome
their
depression,
lack
of
stability,
sexual
and
social
problems
(cited
in
Moshtagh,
2007).
Hess
et
al
(2014)
examined
119
females
in
Germany
and
65.7%
of
those
female
patients
were
satisfied
with
their
life
five
years
after
the
operation.
In
another
study
Tiffiny
(2010)
worked
on
247
(MTF)
patients
and
found
that
their
quality
of
life
was
developed
and
significantly
improved.
Ruppin
(2015)
conducted
a
follow-up
study
and
found
that
71
patients
with
gender
dysphoria
after
10
to
24
years
could
develop
their
social
welfare
and
found
a
job.
Thus
their
life
was
comfortable
and
they
were
satisfied
with
their
interpersonal
and
sexual
relations.
These
patients
are
satisfied
when
they
have
the
operation
since
their
physical
and
mental
situations
become
parallel
and
enjoy
having
their
identity
and
self-confidence
(Ceglie,
2000).
However,
there
are
some
reasons
why
they
did
not
reach
satisfaction,
they
may
face
some
physical
problems
like
the
operation
and
physical
pain,
and
not
having
an
altered
face
or
voice
can
affect
their
behaviors.
These
problems
may
limit
their
life
and
bring
them
depression
(Michel,
2002).
Moreover,
after
the
surgery,
they
may
face
lack
of
beauty
which
is
the
goal
for
female
patients
(DeCupere,
2006).
Other
problems
like
lack
of
relationships
with
the
family
members
and
the
other
people
and
isolation
may
affect
their
life
and
make
them
depressed.
Some
families
do
not
understand
these
patients.
Studies
(e.g.,
Cohen,
1999)
show
that
they
have
strict
and
disciplined
parents
who
reject
these
patients.
In
Iran,
about
70%
of
families
are
angry
with
their
children
who
want
to
talk
about
their
gender
dysphoria
(Rahimi
Ahmadabadi,
2016).
This
may
affect
the
patients’
mental
status.
Lack
of
family
and
friends’
support
with
the
lack
of
medical
treatment
depresses
these
patients
even
after
the
operation.
Family
should
believe
their
problems
since
their
family
may
have
some
wrong
pre-supposed
ideas
(Parola,
2010).
This
can
be
improved
through
family
and
social
support
which
help
the
patients
to
overcome
their
gender
problems
(Besharat,
2012).
The
other
problem
is
that
the
patients
may
not
receive
what
they
perceived
before.
The
patients
who
are
married
and
then
do
the
operation
may
be
divorced
and
lose
their
children.
This
causes
them
to
feel
stress,
anxiety
and
disappointed
status
(Mohr,
2008).
This
situation
can
be
worse
since
Iran
is
a
religious
country
which
follows
some
cultural
values
(Asgari,
2007).
This
study
dealt
with
the
variable
of
patients’
gender,
education
and
occupation
which
showed
no
significant
difference
between
the
operated
and
non-operated
patients.
But
there
is
a
significant
relationship
between
age
and
depression
among
the
operated
participants.
In
other
words,
the
patients
who
had
the
operation
faced
higher
levels
of
depression
in
accordance
with
their
age.
This
may
be
due
to
Iranian
cultural
and
social
situations
which
affect
the
patients’
lives.
Social
and
cultural
positions
may
affect
their
educational
and
social
activities
in
a
very
limited
manner.
They
also
cannot
find
their
partner
easily
and
the
lack
of
stability,
especially
when
they
become
older
may
make
the
depression
more
severe.
In
fact,
people’s
negative
view
on
gender
dysphoria
in
Iran
causes
these
problems
at
the
social
and
cultural
level.
Thus
these
patients
are
depressed
and
mentally
retarded.
Lack
of
family
and
social
support
after
the
treatment
may
be
the
main
reason
for
the
stability
of
the
depression
even
after
the
operation.
Thus
operation
is
not
enough
by
itself.
There
is
a
need
for
consultants,
social
and
family
support,
cultural
and
religious
acceptance.
Psychoanalysis
and
psychological
treatment
are
also
needed
(Michel,
2002).
The
investigation
of
such
problems
mentioned
above
can
improve
the
patients’
feelings
before
and
after
the
operation
(Norian,
2008).
This
can
give
them
an
ordinary
life
which
helps
them
to
be
active
in
the
physical,
mental
and
social
activities
like
other
people
in
the
society.
Acknowledgment
This
article
was
extracted
from
the
project
confirmed
by
Abadan
School
of
Medical
Sciences
with
the
code
of
95St-0071
and
ethical
code
of
IR.ABADANUMS.REC.1395.102
.The
authors
thank
all
the
officials
who
did
financial
support
and
the
patients
who
took
part
in
the
present
study.
Ceglie,
D.
D.
Gender
Identity
Disorder
in
Young
People.
Journal
of
Advances
in
Psychiatric
Treatment
2000;
(6):
458-466.
Correll
S.
H.J.,
Byrne
D.
Gender
and
career
process:
The
role
of
based
self-assessments.
American
journal
of
sociology
2001;
106(6):
1691-1730.
Sadock
B,
Sadock
V,
Ruiz
P.
Comprehensive
Text
of
Psychiatry.
Ninth
edition,
volume
1,
2009
Tavassoli
A,
Hassanian
A,
Saber
SM.
Social
factors
expediting
sex
change
surgery
in
patients
with
gender
Identity
Disorders.
Journal
of
Forensic
Medicine
Iran2014;
2(20):19-26.
Putnam
F.
Ten-year
research
update
review:
child
sexual
abuse.
Journal
of
the
academy
of
child
adolescent
and
psychiatry
2003;
42:
269-278.
Putnam
F.
Ten-year
research
update
review:
child
sexual
abuse.
Journal
of
the
academy
of
child
adolescent
and
psychiatry
2003;
42:
269-278.
Veale
JF,
Clarke
DE,
Lomax
TC.
Biological
and
psychosocial
correlates
of
adult
gender-variant
identities:
A
review.
Personality
and
Individual
Differences.
2010;
48:
357-366.
Sohn
M,
Bosinski
H.
Gender
identity
disorders:
diagnostic
and
surgical
aspects.
Journal
of
Sex
Med
2007;
4:
1193-1208.
Hepp
U,
Kraemer
B,
Schnyder
U,
Miller
N,
Delsignore
A.
Psychiatric
comorbidity
in
gender
identity
disorder.
Journal
of
psychosomatic
research
2005;
58:
259-261.
Matsumoto
Y,
Sato
T,
Ohnishi
M,
Kishimoto
Y,
Terada
S,
Kuroda
Sh.
Stress-coping
strategies
of
patients
with
gender
identity
disorder.
Psychiatry
Clin
Neurosci
2009;
63(6):715-20.
American
Psychiatric
Association.
Diagnostic
References
and
Statistical
Manual
of
Mental
Disorders
(Fourth
Edition)
Text
Revision.
(DSM-IV-TR).
Washington
DC:
APA,
2000.
Gomez-Gile
E,
Zubi
aurre-
Elorza
L,
Isabel
E,
Guillamon
A,
Godas
T,
Almaraz
M.C
and
et
al.
Hormone
–treated
transsexuals
report
less
social
distress
anxiety
and
depression.
Psychoneuroendocrinology
2012;
37:
662-670.
Rahimi
Ahmadabadi
S,
Hejazi
A,
Ataran
H,
Rahimi
A,
Kohestani
L,
Karashki
H,
Aghamohamdian
H.
Comparison
of
stress,
anxiety,
Depression
&
sexual
role
in
subjects
involved
gender
dysphoria
with
normal
subjects.
Iranian
Journal
of
Forensic
Medicine
2016;
22(1):
67-75.
Cook
K
J.
Gender
identity
disorders:
A
misunderstood
diagnosis.
In
partial
fulfillment
of
the
requirements
for
the
degree
of
Master
of
Arts
sociology.
Marshall
University
2004.
Norian
N,
Dolatshahi
B,
Rezaee
A.
Study
of
personality
disorders
and
personality
characteristics
of
men
with
gender
identity
disorder.
Rehabilitation2008;
9(1):
55-60.
Lothstein
L
M.
The
postsurgical
transsexual:
empirical
and
theoretical
considerations.
Archive
of
Sexual
Behavior1980;
9:
547-64.
Besharat
M
A,
Tolaeean
F,
Gholamali
lavasani
M.
Comparison
of
attachment
styles
in
gender
identity
disorder
patients
and
non-patients
.Journal
of
Forensic
Medicine
Iran
2012;
18(2-3):
89-97.
Rakic
Z,
Starcevice
V,
Maric
J,
Kelin
K.
The
outcome
of
sex
reassignment
surgery
in
Belgrade:
32
patients
of
both
sexes.
Archive
of
Sexual
Behavior1996;
25:
515-525.
Ainsworth,
T
A,
Spiegel
J
H.
Quality
of
life
individuals
with
and
without
facial
feminization
surgery
or
gender
reassignment
surgery.
Qual
life
Res
2010;
19(7),
1019-1024.
Lief
H,
Hubschman
L.
Orgasm
in
postoperative
transsexual.
Archive
of
Sexual
Behavior
1993;
22:
145-55.
Gorin-Lazard
A,
Baumstarck
K,
Boyer
L,
Maquigneau
A,
Gebleux
S,
Penochet
JC,
et
al.
Is
hormonal
therapy
associated
with
better
quality
of
life
in
transsexuals?
A
cross-sectional
study.
J
Sex
Med
2012;
9(2):531-41.
Michel
A,
Ansseau
M,
Legros
J.J.,
Pitchot
W,
Mormont
C.
The
transsexual:
what
about
the
future?
European
Psychiatry
2002;
17(6):353-362.
Asgari
M,
Saberi
M,
Dolatshahi
B.
The
prevalence
of
psychological
damage
in
patients
with
GID.
Journal
of
Forensic
Medicine
Iran
2007;
13(3):
181-186.
javaheri
F,
Koochakian
Z.
GID
&
Its
Social
Dimensions:
Review
of
the
Phenomenon
of
Sexual
Dissatisfaction
in
Iran.
Journal
of
Social
Science:
Social
Welfare
2006;
21:
265-292.
Beck
A
T,
Steer
R
A,
Brown
GK.
Manual
of
the
Beck
inventory-II.
San
Antonio
TX:
The
Psychological
Corporation;
2000.Beck
AT,
Steer
R
A.
Internal
consistencies
of
the
original
and
revised
beck
depression
inventory.
Journal
of
clinical
Psychology
1984;
40(6):
1364-1367.
Shafer
A
B.
Meta-analysis
of
the
factor
structures
of
four
depression
questionnaires:
Beck,
CES-D,
Hamilton,
and
Zung.
Journal
of
Clinical
Psychology
2006;
62(1):123-146.
Nuevo
R,
Dunn
G,
Dowrick
C,
Vázquez-Barquero
J.L.,
Casey
P,
Dalgard
O.S,
Lehtinen
V
&
et
al.
Cross-cultural
equivalence
of
the
Beck
Depression
Inventory:
A
five-country
analysis
from
the
ODIN
study.
Journal
of
Affective
Disorders
2009;
114(1-3):
156-162.
Alto
A
M,
Elovainio
M,
Kivimaki
M,
Uutela
A,
Sami
P.
The
Beck
Depression
Inventory
and
General
Health
Questionnaire
as
measures
of
depression
in
the
general
population:
A
validation
study
using
the
Composite
International
Diagnostic
Interview
as
the
gold
standard.
Psychiatry
Research
2012;
197(1-2):
163-171.
De
Cuypere
G,
Elaut
E,
Heylens
G,
Van
Maele
G,
Selvaggi
G,
T’Sjoen
G,
et
al.
Long-term
follow-up:
Psychological
outcome
of
Belgian
transsexuals
after
sex
reassignment
surgery.
Sexologies
2006;
15(2):
126-133.
Parola
N,
Bonierbale
M,
Lemaire
A,
Aghababian
V,
Michel
A,
Lancon
C.
Study
of
quality
of
life
for
transsexuals
after
hormonal
and
surgical
reassignment.
Sexologies
2010;
19:
24-8.
Moshtagh
N.
Are
there
only
two
Genders?
Baztab
Danesh
a
journal
of
Cognition,
Brain
and
Behavior
2007;
1:
32-34.
Hess
J,
Neto
R
R,
Panic
L,
Rubben
H,
Sewf
W.
Satisfaction
with
male-to-female
gender
reassignment
surgery.
Dutsches
Arzteblatt
International
2014;
111:795-801.
Cohen
P
T,
Gooren
J.G.
Transsexualism.
Journal
of
psychosomatic
research
1999;
46(4):315-333.
Mohr
J.
Attachment
in
adolescence
and
adulthood.
In
hand
book
of
attachment.
Second
edition,
edited
by
Cassidy
J,
Shaver
P.
The
Guilford
Press,
New
York
London
2008
Afkar
AH,
Mahboubi
M,
Shahri
MN,
Mohamadi
M,
Jalilian
F,
Moradi
F.
Investigation
of
the
Relationship
between
Illogical
Thoughts
and
Dependence
on
Others
and
Marriage
Compatibility
in
the
Iranian
Veterans
Exposed
to
Chemicals
in
Iran-Iraq
War.
Global
Journal
of
Health
Science.
2014;6(5):274-9.
Cardoso
da
Silva
D,
Schwarz
K,
Fontanari
A.M.,
Costa
A.B.,
Massuda
R,
Henriques
A.A.,
Salvador
J,
Silveira
E,
Elias
Rosito
T,
Lobato
M.I
.WHOQOL-100
Before
and
After
Sex
Reassignment
Surgery
in
Brazilian
Male-to-Female
Transsexual
Individuals.
J
Sex
Med
2016;
13(6):988-993.
Tiffiny
A,
Jeffrey
H.
Quality
of
life
of
individuals
with
and
without
facial
feminization
surgery
or
gender
reassignment
surgery.
Quality
of
Life
Research
2010;
19(7):
1019-1024.
Reisner
S
L,
Biello
K
B,
White
Hughto
J.M,
Kuhns
L,
Mayer
K.H,
Garofalo
R,
Mimiaga
M.J.
Psychiatric
Diagnoses
and
Comorbidities
in
a
Diverse,
Multicity
Cohort
of
Young
Transgender
Women:
Baseline
Findings
from
Project
Life
Skills.
JAMA
Pediatric
2016;
170(5):
481-486.
Gómez-Gila
E,
Vidal-Hagemeijera
A,
Salameroa
M.
MMPI–2
Characteristics
of
Transsexuals
Requesting
Sex
Reassignment:
Comparison
of
Patients
in
Prehormonal
and
Presurgical
Phases.
Journal
of
Personality
Assessment
2008;
90(4):
368-374.
Ruppin
U,
Pfäfflin
F.
Long-Term
Follow-Up
of
Adults
with
Gender
Identity
Disorder.
Arch
Sex
Behav2015;
44(5):1321-9.
Campo
J,
Nijman
H.
Psychiatric
Co
morbidity
of
Gender
Identity
Disorders.
The
American
Journal
of
Psychiatry
2003;
160:1332-36
|

