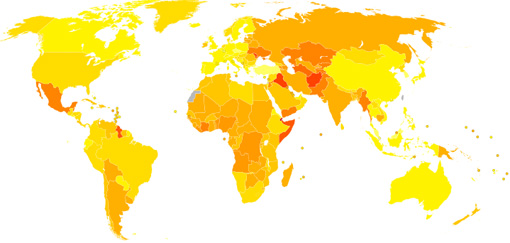
Most
severe
congenital
anomalies
occur
in
low-
and
middle-income
countries
(1).
The
following
summarises
the
major
causes:
1.
Diet
and
appropriate
nutrition
Being
born
in
a
low
income
or
developing
nation
can
have
an
immediate
effect
on
risk
factors
not
only
through
malnourishment
of
the
mother
and
consequently
the
foetus,
but
also
lack
of
dietary
requirements
and
inability
to
afford
supplements.
1a.
Folate
An
adequate
intake
of
folate
in
the
peri-conceptional
period
has
the
capacity
to
prevent
70
per
cent
of
all
cases
of
Neural
Tube
Defects
(NTD).
Those
women
planning
pregnancy
are
therefore
in
a
position
to
avoid
such
defects
by
ensuring
adequate
supplies
in
their
diet.
For
women
unable
to
purchase
folate
supplements
it
is
readily
found
in
green
leafy
vegetables.
The
growing
and
eating
of
such
vegetables
is
a
cost
effective
way
of
avoiding
NTD.
Neural
tube
defects
include
spina
bifida,
encephalocoele
and
anencephaly,
and
result
from
failure
of
the
spinal
cord
or
brain
to
develop
normally
during
early
foetal
development.
Less
than
40
per
cent
of
those
affected
survive
to
birth.
People
born
with
an
NTD,
especially
those
with
spina
bifida,
will
experience
lifelong
disability.
Pregnancy
guidelines
recommend
that
women
of
childbearing
age
take
in
0.5mg
of
folic
acid
for
at
least
one
month
before
pregnancy
and
three
months
into
the
pregnancy.
Women
who
are
at
high
risk
of
having
a
baby
with
an
NTD
include
those
where
a
parent-to-be
has
spina
bifida,
has
had
a
previous
child
with
an
NTD,
has
a
close
relative
with
an
NTD,
or
where
the
woman
has
been
treated
for
epilepsy.
These
women
should
take
ten
times
the
minimal
dose
(5mg
of
folic
acid
daily
one
month
before
pregnancy
and
three
months
into
the
pregnancy)
(2).
1b.
Vitamin
requirements
Vitamin
A
deficiency
may
cause
blindness
while
excessive
vitamin
A
intake
during
pregnancy
may
affect
the
normal
development
of
an
embryo
or
foetus.
Risk
of
Vitamin
D
deficiency
can
be
found
in
those
with
low
exposure
to
sunlight
(this
may
include
Muslim
women
whose
attire
can
prevent
adequate
sunlight
exposure),
in
women
with
dark
skin,
and
those
with
a
pre
pregnancy
BMI
40.
Vitamin
D
deficiency
leads
to
a
higher
risk
of
pregnancy
complications
such
as
gestational
diabetes,
preeclampsia,
preterm
birth,
and
low
birth
weight
(3).
The
new
Australian
study
outlined
below
shows
that
lack
of
Vitamin
B
may
be
the
cause
of
many
of
the
50%
of
unexplained
congenital
anomalies.
The
obvious
conclusion
from
these
studies
is
that
pregnant
women
need
to
have
a
varied
diet
that
covers
all
food
groups,
vitamins
and
minerals,
to
allow
the
foetus
to
gain
all
it
needs
for
proper
development.
This
obviates
the
necessity
of
nutritional
guidelines
and
prenatal
care
being
made
available
to
all
pregnant
women
globally.
2.
Pre-natal
care
Prenatal
care
should
not
only
include
guidelines
as
to
a
healthy
diet
for
mother
and
foetus,
but
also
the
monitoring
of
foetal
growth
and
mother’s
health;
for
example,
for
cases
of
gestational
diabetes,
eclampsia
and
pre
eclampsia
.
Mothers
in
low
socio-economic
areas
may
receive
no
pre-natal
care
at
all,
as
well
as
be
subject
to
a
wider
range
of
causative
factors.
In
some
developed
countries
the
foetus
or
mother
is
screened
for
congenital
and
genetic
disorders
and
aborted
if
found
to
be
affected
or
a
genetic
carrier.
3.
Vaccination,
Infection
and
disease
A
number
of
maternal
diseases
are
known
to
cause
congenital
anomalies
with
the
most
common
being
syphilis
and
rubella.
Rubella
vaccination
of
women
and
girls
occurs
in
most
developed
nations
but
is
a
more
prevalent
cause
of
congenital
anomalies
in
low-
and
middle-income
countries.
More
recently,
the
effect
of
in
utero
exposure
to
Zika
virus
has
been
reported
and
has
had
devastating
congenital
defects,
such
as
severe
microcephaly,
subcortical
calcification,
congenital
contractures
and
hypertonia,
and
is
now
prevalent
in
a
wide
range
of
countries
that
host
the
mosquito
carrier
(4).
4.
Environmental
risks
While
there
can
be
a
wide
range
of
environmental
dangers
to
the
developing
foetus,
such
as
infections
and
disease
prevalence,
maternal
exposure
to
certain
pesticides,
chemicals,
and
medications
(including
traditional
herbal
mixtures),
alcohol,
tobacco
and
radiation
during
pregnancy,
increases
the
risk
of
congenital
anomalies.
Working
or
living
near,
or
in,
waste
sites,
smelters
or
mines
may
also
be
a
risk
factor
(1).
These
risk
factors
are
more
common
in
low
and
middle
income
countries.
5.
Genetic
factors
These
can
be
inherited
conditions
such
as
anophthalmos,
microphthalmos,
coloboma,
congenital
cataract,
infantile
glaucoma,
and
neuro-ophthalmic
lesions
as
examples.
Complicating
inherited
genetic
disorders
are
issues
of
consanguinity.
This
can
be
a
primary
cause
where
consanguinity
increases
the
prevalence
of
rare
genetic
congenital
anomalies
and
nearly
doubles
the
risk
for
neonatal
and
childhood
death,
intellectual
disability
and
other
anomalies
(5).
The
high
prevalence
of
consanguinity
in
some
regional
areas
needs
a
thoughtful
public
health
approach.
Vaccination,
appropriate
diet,
including
adequate
intake
of
folic
acid
or
iodine
through
fortification
of
staple
foods
or
supplementation,
including
the
Vitamins
groups
discussed
here,
in
addition
to
adequate
prenatal
care,
are
necessary
prevention
methods.
Doctors
everywhere
also
need
to
be
alert
to
viral
outbreaks
and
higher
incidence
of
anomalies
in
their
patient
populations,
report
such
to
health
authorities
and,
ideally,
investigate
the
causes
(6).
| REPORT
ON
AUSTRALIAN
RESEARCH
|
Australian
researchers
in
a
12
year
study,
have
recently
published
evidence
that
supplements
of
vitamin
B-3
can
prevent
many
miscarriages
and
congenital
defects
(7).
A
team
of
researchers
has
identified
a
key
factor
behind
some
miscarriages
and
congenital
malformations
of
the
heart,
spine,
kidneys,
and
cleft
palate.
The
Australian
study
evaluated
the
cause
of
a
number
of
abnormal
embryonic
developments
to
a
deficiency
in
nicotinamide
adenine
dinucleotide
(NAD),
a
molecule
that
plays
a
key
role
in
metabolic
regulation.
NAD
is
involved
in
energy
production
and
boosting
cell
survival,
as
well
as
supporting
DNA
repair.
However,
NAD
production
canbe
inhibited
by
some
genetic
factors,
chronic
diseases
(such
as
diabetes),
or
an
unhealthy
diet,
leading
to
NAD
deficiency.
The
study
initially
focused
on
families
exhibiting
a
rare
condition
known
by
its
acronym
as
“VACTERL.”
This
condition
refers
to
people
born
with
at
least
three
of
the
following
anomalies:
vertebral
defects,
anal
atresia,
cardiac
defects,
tracheo-esophageal
fistula,
renal
anomalies,
or
limb
abnormalities.
The
researchers
found
that
a
shortage
of
NAD
in
these
families
resulted
in
miscarriages
or
birth
defects.
They
also
concluded
that
NAD
deficiency
might
therefore
explain
a
wider
range
of
miscarriage
and
congenital
anomalies
globally.
The
research
indicated
that
a
relatively
simple
solution
in
preventing
such
disorders
was
ensuring
required
Vitamin
B-3
intake.
They
found
a
key
element
in
NAD
synthesis
is
niacin,
a
vitamin
B-3
complex
available
as
a
dietary
supplement
(7).
A
sustained
intake
of
B-3
complex
supplements,
the
researchers
suggest,
can
effectively
prevent
miscarriages
and
birth
defects
such
as
spina
bifida
and
other
vertebral
segmentation
malformations,
as
well
as
some
heart
and
small
kidney
defects.
An
earlier
Australian
study
(8)
found
vitamin
B-3
deficiencies
in
mothers
already
taking
B-3
supplements.
Appropriate
intake
of
vitamin
B-3
during
the
first
trimester
is
a
requirement
for
proper
organ
development
in
the
developing
foetus
(8).
This
may
indicate
that
pregnant
women
require
an
even
higher
vitamin
B-3
intake.
The
Australian
study
evaluated
the
effect
of
niacin
on
developing
embryos
in
a
preclinical
mouse
model,
and
noted
that,
after
the
vitamin
B-3
complex
was
appropriately
introduced
into
the
expecting
mother’s
diet,
miscarriages
no
longer
occurred.
Moreover,
all
the
babies
were
born
healthy,
with
no
congenital
malformations.
They
used
genomic
sequencing
to
identify
potentially
pathogenic
gene
variants
in
families
in
which
a
person
had
multiple
congenital
malformations
and
tested
the
function
of
the
variant
by
using
assays
of
in
vitro
enzyme
activity
and
by
quantifying
metabolites
in
patient
plasma.
Variants
were
identified
in
two
genes.
The
researchers
say
that
developing
a
test
to
measure
levels
of
NAD
in
expecting
mothers
will
come
next.
This
will
allow
practitioners
to
identify
which
women
risk
miscarriage
or
delivering
a
baby
with
a
congenital
malformation,
and
who
therefore
need
to
take
more
B-3
supplements
in
pregnancy.
For
the
time
being,
expectant
mothers
should
include
Vitamin
B-3
foods
in
their
regular
diet
but
only
take
B-3
supplements
as
advised
by
their
doctors,
as
it
is
still
unclear
what
exact
doses
of
vitamin
B-3
would
help
to
prevent
miscarriages
and
malformations
in
each
case.
The
current
required
daily
intake
of
Niacin
(Vitamin
B3)
is
20mg
(2).
Niacin
or
Vitamin
B3
is
an
essential
vitamin
for
human
health
that
processes
fat
in
the
body,
regulates
blood
sugar
levels
and
lowers
cholesterol
levels.
A
deficiency
of
niacin
causes
symptoms
of
diarrhoea,
dermatitis,
dementia,
inflammation
of
the
mouth,
amnesia,
delirium,
and
if
untreated,
death.
It
is
found
in
many
foods
(see
Table
1).
Table
1:
Niacin
containing
foods
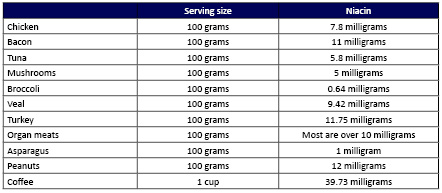
Data
Source:
NHMRC
(2).