|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
........................................................
|
|
Original contribution/Clinical Investigation
Diabetes Mellitus
- Knowledge, Management and Complications: Survey
report from Faisalabad-Pakistan
Ijaz Anwer, Ahmad Shahzad, Kashmira Nanji, Farah
Haider, Muhammad Masood Ahmad
Alanine aminotransferase
indicates excess weight and dyslipidemia
Mehmet Rami Helvaci, Orhan Ayyildiz* Mustafa
Cem Algin, Yusuf Aydin, Abdulrazak Abyad, Lesley
Pocock
Comparative Analysis of Antimicrobial Peptides
Gene Expression in Susceptible/Resistant Mice
Macrophages to Leishmania major Infection
Hamid Daneshvar, Iraj Sharifi, Alireza Kyhani,
Amir Tavakoli Kareshk, Arash Asadi
Does
socio-economic status of the patients have effect
on clinical outcomes after coronary artery bypass
grafting surgery?
Forough Razmjooei, Afshin Mansourian, Saeed
Kouhpyma
Comparison of the uterine
artery Doppler indices during pregnancy between
gestational diabetes and diabetes mellitus and
healthy pregnant women
Nazanin Farshchian, Farhad Naleini, Amir Masoud
Jaafarnejhad,
Parisa Bahrami Kamangar
Survey single dose
Gentamicin in treatment of UTI in children with
range of 1 month to 13 years old in Jahrom during
2015
Ehsan Rahmanian, Farideh Mogharab,
Vahid Mogharab
Evaluation of control of
bleeding by electro cauterization of bleeding
points of amplatz sheath tract after percutaneous
nephrolithotomy (PCNL) in Jahrom Peymanieh hospital
during year 2015-2016
Ali Reza Yousefi , Reza Inaloo
Comparison of the three-finger
tracheal palpation technique with triple ID
formula to determine endotracheal tube depth
in children 2-8 years in 2016-2017
Anahid Maleki, Alireza Ebrahim Soltani, Alireza
Takzare, Ebrahim Espahbodi,
Mehrdad Goodarzi , Roya Noori
Effect of Sevoflurane
and Propofol on pulmonary arterial pressure
during cardiac catheterization in children with
congenital heart diseases
Faranak Behnaz, Mahshid Ghasemi , Gholamreza
Mohseni, Azim Zaraki
Population and Community Studies
Prevalence
and risk factors of obesity in children aged
2-12 years in the Abu Dhabi Islands
Eideh Al-Shehhi, Hessa Al-Dhefairi, Kholoud
Abuasi, Noora Al Ali, Mona Al Tunaiji, Ebtihal
Darwish
Study and comparison
of psychological disorders in normal students
and students with multiple sclerosis in Shahrekord
Neda Ardestani-Samani, Mohammad Rabiei, Mohammad
Ghasemi-Pirbalooti, Asghar Bayati, Saeid Heidari-Soureshjani
Comparative
study of self-concept, physical self-concept,
and time perspective between the students with
multiple sclerosis and healthy students in Shahrekord
Neda Ardestani-Samani, Mohammad Rabiei, Mohammad
Ghasemi-Pirbalooti, Asghar Bayati, Saeid Heidari-Soureshjani
Relationship
between Coping Styles and Religious Orientation
with Mental Health in the Students of the Nursing-Midwifery
Faculty of Zabol
Nasim Dastras, Mohsen Heidari Mokarrar, Majid
Dastras, Shirzad Arianmehr
Tuberculosis in Abadan,
Iran (2012-2016): An Epidemiological Study
Ali-Asghar ValiPour, Azimeh Karimyan, Mahmood
Banarimehr, Marzieh Ghassemi, Maryam Robeyhavi,
Rahil Hojjati,
Parvin Gholizadeh
Family Stability and Conflict
of Spiritual Beliefs and Superstitions among
Yazdi People in Iran: A Qualitative Study
Zahra Pourmovahed , Seyed Saied Mazloomy Mahmoodabad
; Hassan Zareei Mahmoodabadi ; Hossein Tavangar
; Seyed Mojtaba Yassini Ardekani ; Ali Akbar
Vaezi
A comparative
study of the self-actualization in psychology
and Islam
Simin Afrasibi, Zakieh Fattahi
The effectiveness
of cognitive - behavioral therapy in reducing
the post-traumatic stress symptoms in male students
survivors of earthquake in the central district
of Varzeghan
Sakineh Salamat, Dr.Ahad Ahangar, Robab Farajzadeh
Reviews
Effects and mechanisms
of medicinal plants on stress hormone (cortisol):
A systematic review
Kamal Solati, Saeid Heidari-Soureshjani, Lesley
Pocock
Comparing Traditional
and medical treatments for constipation : A
Review Article
Mohammad Yaqub Rajput
A review of anti-measles
and anti-rubella antibodies in 15- 25 year old
women in Jahrom City in 2011
Ehsan Rahmania , Farideh Mogharab, Vahid Mogharab
Review of percutaneous
nephrolithotomy in children below 12 years old
in Jahrom hospital, during 2010-2014
Ali Reza Yousefi , Reza Inaloo
Physical and
mental health in Islam
Bahador Mehraki, Abdollah Gholami
International Health Affairs
The Challenges of Implementation
of Professional Ethics Standards in Clinical Care
from the viewpoint of Nursing Students and Nurses
Saeedeh Elhami, Kambiz Saberi, Maryam Ban, Sajedeh
Mousaviasl, Nasim Hatefi Moadab, Marzieh Ghassemi
Cognitive Determinants
of Physical Activity Intention among Iranian Nurses:
An Application of Integrative Model of Behavior
Prediction
Arsalan Ghaderi, Firoozeh Mostafavi, Behzad Mahaki,
Abdorrahim Afkhamzadeh,
Yadolah Zarezadeh , Erfan Sadeghi
Effect of resilience-based
intervention on occupational stress among nurses
Hossein Jafarizadeh, Ebrahim Zhiyani, Nader
Aghakhani, Vahid Alinejad, Yaser Moradi
Education and Training
Calculation of Salaries
and Benefits of Faculty Members in the Ministry
of Health and Medical Education of Iran
Abdolreza Gilavand
The effect of education
on self-care behaviors of gastrointestinal side
effects on patients undergoing chemotherapy
Shokoh Varaei, Ehsan Abadi Pishe, Shadan Pedram
Razie, Lila Nezam Abadi Farahani
Creating and
Validating the Faith Inventory for Students
at Islamic Azad University of Ahvaz
Solmaz Choheili, Reza Pasha, Gholam Hossein
Maktabi, Ehsan Moheb
Creating
and Validating the Adjustment Inventory for
the Students of Islamic Azad University of Ahvaz
Homa Choheili, Reza Pasha, Gholam Hossein Maktabi,
Ehsan Moheb
Evaluating
the Quality of Educational Services from the
Viewpoints of Radiology Students of Ahvaz Jundishapur
University of Medical Sciences
Abdolreza Gilavand, Jafar Fatahiasl
An Investigation
of Psychosocial aspect of Iranian Nursing Students'
Clinical Setting
Mahsa Boozaripour , Zanyar Karimi, Sima Zohari
Anbohi, Amir Almasi-Hashiani, Fariba Borhani
Clinical Research and Methods
Comparison of the
Antibacterial Effects of Chlorhexidine Mouth
washes with Jaftex Mouth wash on Some Common
Oral Microorganisms (An in Vitro Study)
Ebrahim Babadi, Zahra Bamzadeh, Fatemeh Babadi
Study of the effect
of plasma jet on Fusarium isolates with ability
to produce DON toxins
Elham Galin Abbasian, Mansour Bayat, Arash chaichi
Nosrati, Seyed Jamal Hashemi, Mahmood Ghoranneviss
The comparison of
anti-inflammatory effect in two methods of topical
dexamethasone injection and topical application
of ginger alcoholic extract after removing mandibular
wisdom teeth
Sahar Zandi, Seyyed Muhammadreza Alavi, Kamran
Mirzaie, Ramin Seyedian, Narges Aria, Saman
Jokar
The effect of curcumin
on growth and adherence of major microorganisms
causing tooth decay
Leila Helalat, Ahmad Zarejavid, Alireza Ekrami,
Mohammd Hosein Haghighizadeh, Mehdi Shiri Nasab
|
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| November 2017
- Volume 15, Issue 9 |
|
|
Review of percutaneous
nephrolithotomy in children below 12 years old
in Jahrom hospital, during 2010-2014
Ali Reza Yousefi
Reza Inaloo
Department of Urology, Jahrom University of
Medical Sciences, Jahrom, Iran.
Corresponding author:
Reza Inaloo, Department of Urology,
Jahrom University of medical sciences,
Jahrom, Iran
Tel: +989173130056
Email: rezainaloo@yahoo.com
|
Abstract
Introduction: Although,
renal stone isn’t frequent in children,
but Percutaneous Nephrolithotomy can be
used in children if indicated. Percutaneous
Nephrolithotomy in children is different
from adults, thus we review some children
who underwent Percutaneous Nephrolithotomy
and review them for complications and
stone free rate.
Material and
Methods: This study was done using
descriptive cross-sectional method on
43 cases under 12 years old who had renal
stone and were treated by Percutaneous
Nephrolithotomy in Jahrom Peymanieh hospital.
All cases had medical records. Having
a renal stone larger than 2cm, multiple
stone, no response to extra corporeal
shock wave lithotripsy were a criteria
for patients below 12 years old to be
involved in the study and to be cured
by Percutaneous Nephrolithotomy operation.
Patient’s data was collected with
a research made questionnaire.Data was
investigated in a level of descriptive
statistics via statistics software (SPSS,
Edition14) in which the average and deviation
of criteria and qualitative variables
from frequency percentage and frequency
was used in quantitative variables of
descriptive reports.
Results:
From 43 patients 22 patients (51.1%) were
male and 21 patients (48.8%) were female.
The patients were aged from 7 months to
11 years old. The stone size ranged from
1cm to 2.5 cm. The number of stones in
42 patients had been recorded. Among these
45.2 percent of them had one stone and
33.3 percent had two. The stone free rate
was 85%. The average of hospital stay
was 31.11±12.56 hours. The longest
time was 24 and 48 hour andthat respectively
included 33.3% and 26.2%. The complications
were: (0%), Excessive bleeding which needed
transfusion (0%), post op convulsion (9.5%),
and organ injury (0%).
Discussion:
Percutaneous stone therapy-related
hemorrhage requires a blood transfusion
(11%-14%), and an increased risk of kidney
loss. In this study, the stones were removed
completely with minimal injury to renal
tissue. PCNL has a better stone clearance
rate and is cost-effective. PCNL has a
clearance rate of 100% when it was combined
with ESWL.
Key words:
Percutaneous Nephrolithotomy, Renal
stone, Pediatrics
|
Nephrolithiasis is a common clinical disorder
affecting up to 5% of the general population
in the USA [1]. The prevalence of renal stone
disease has been rising in both sexes, being
estimated that about 5% of American women and
12% of men will develop a kidney stone at some
time in their life [2]. Nevertheless, in certain
areas of the world, as in the Middle East, the
lifetime risk appears to be even higher [3].
There has been heightened awareness of renal
stone disease in children as well [4]. Recurrence
rates of 50% after 10 years and 75% after 20
years have been reported [56]. Clinical manifestations
are characterized by lumbar pain of sudden onset
[the location of pain depends on the location
of the stone in the urinary tract] which may
be accompanied by nausea and vomiting, and gross
or microscopic hematuria Diagnosis of renal
stone in the acute setting is beyond the scope
of the present update but in brief, is represented
by urinalysis and imaging. Urinalysis often
reveals hematuria but the latter is absent in
approximately 9% of cases [3]. Crystal Luria
is occasional and the presence of leucocyturia
may suggest associated urinary tract infection.
Unenhanced helical computed tomography [CT]
scan, the most sensitive and specific radiographic
test, is becoming the diagnostic procedure of
choice to confirm the presence of kidney and
especially of ureteral stones [4].Renal colic
must be differentiated from musculoskeletal
pain, herpes zoster, pyelonephritis, appendicitis,
diverticulitis, acute cholecystitis, gynecologic
disease, ureteral stricture of obstruction due
to blood clot, and polycystic kidney disease
[5]. Stone formation usually results from an
imbalance between factors that promote urinary
crystallization, and those that inhibit crystal
formation and growth [5]. Urinary tract stone
disease is likely caused by 2 basic phenomena.
The first phenomenon is supersaturating of the
urine by stone forming constituents, including
calcium, oxalate, and uric acid. Crystals or
foreign bodies can act as nidi, upon which ions
from the supersaturated urine form microscopic
crystalline structures. The overwhelming majority
of renal calculi contain calcium [6]. Other,
less frequent stone types include cysteine,
ammonium acid urate, xanthine, dihydroxyadenine,
and various rare stones related to precipitation
of medications in the urinary tract. Stones
of the upper urinary tract are more common in
the United Stated than in the rest of the world.
Roughly 2 million patients present on an outpatient
basis with stone disease each year in the United
States, which is a 40% increase from 1994[12].
The incidence of urinary tract stone disease
in developed countries is similar to that in
the United States. Stone disease is rare in
only a few areas, such as Greenland and the
coastal areas of Japan. In developing countries,
bladder calculi are more common than upper urinary
tract calculi; the opposite is true in developed
countries. These differences are believed to
be diet-related [13]. The morbidity of urinary
tract calculi is primarily due to obstruction
with its associated pain, although non obstructing
calculi can still produce considerable discomfort.
Stone- induced hematuria is frightening to the
patient but is rarely dangerous by itself. The
most morbid and potentially dangerous aspect
of stone disease is the combination of obstruction
and upper urinary tract infection. Stones are
more common in hot and dry areas and diet heredity
also appears to be a factor. Stone disease is
much more frequent in whites. In general, urolithiasis
is more common in males. Stone due to discrete
metabolic/hormonal defects, cystinuria, hyperparathyroidism
and stone disease in children are equally prevalent
between the sexes. Stones due to infection [struite
calculi] are more common in women than in men.
Most urinary calculi develop in patients aged
20-49 years. Patients in whom multiple recurrent
stone forms usually develop their first stones
while in their second or third decade of life.
An initial stone attack after age 50 years is
relatively uncommon [14]. Patients with urinary
calculi may report pain, infection, or hematuria.
Small non obstructing stones in the kidneys
only occasionally cause symptoms. The passage
of stones into the ureter with subsequent acute
obstruction, proximal urinary tract dilation,
and spasm is associated with classic renal colic.
Renal colic is characterized by undulating cramps
and severe pain and is often associated with
nausea and vomiting. As the stone travels through
the ureter, the pain moves from the flank to
the upper abdomen, then to the lower abdomen,
down to the groin, and eventually to the scrotal
or labial areas. Associated bladder irritative
symptoms are common when the stone is located
in the distal or intramural ureter. Patients
with large renal stones known as stag horn calculi
are often relatively asymptomatic. Asymptomatic
bilateral obstruction, which is uncommon, manifests
as symptoms of renal failure. Approximately
80% of kidney stones contain calcium, and the
majority of them are composed primarily of calcium
oxalate. Although most calcium oxalate stones
contain some calcium phosphate, only 5% have
hydroxyapatite of brushite as their main constituent
and 10% contain some uric acid [15]. Evaluation
of a renal stone patient starts with a detailed
history focusing on occupation, dietary and
lifestyle habits, previous use of medications,
family predisposition, and history of recurrent
urinary tract infection and underlying disorders
that predisposes to nephrolithiasis [16].
This
study
was
done
using
descriptive-cross-sectional
method
on
43
patients
below
age
of
12,
who
had
been
suffering
from
renal
stone
and
were
treated
by
use
of
PCNL
operation
(percutaneous
Nephrolithomy
procedures)
at
Jahrom
Paymanieh
hospital.
All
the
patients
had
medical
records.
The
study
was
conducted
using
a
form
which
had
been
provided
and
completed
by
the
surgeon.
The
patients
who
under
went
PCNL
had
renal
stone
larger
than
>2cm
or
multiple
stones
or
no
response
to
ESWL.
The
criteria
for
exiting
from
the
study
were
age
above
12
years
old
and
renal
stone
smaller
than
2cm.
(The
information
was
collected
by
the
use
of
a
form
which
had
been
provided
and
completed
by
the
physician).The
mentioned
information
in
the
form
included:
gender
(sex),
age,
place
of
stone,
kind
of
stone,
number
of
stones,
operation’s
side
effects,
the
number
of
remained
stones,
number
of
hemoglobin
after
operation
and
time
of
hospitalization.
(Admission
in
hospital).
This
information
was
included
in
the
questionnaire
by
observing
the
ethics
and
investigation
committee’s
instructions
of
Iran’s
Ministry
of
Health.
Names
and
details
of
participants
were
confident
and
each
patient
was
given
a
numerical
code.
Finally
the
obtained
information
was
investigated
in
a
level
of
descriptive
statistics
via
statistics
software
(SPSS,
Edition14)
in
which
the
average
and
deviation
of
criteria
and
qualitative
variables
from
frequency
percentage
and
frequency
was
used
in
quantitative
variables
of
descriptive
reports.
Research
Method:
At
first,
after
general
anesthesia,
cystoscopy
was
done
by
(stortz
10F)
in
supine
position.
Then
a
urethral
catheter
(5F)
was
sent
within
involved
kidney
and
fixed
Foley
catheter
and
then
in
prone
position,
nephrostomy
needle
was
sent
to
inferior
and
posterior
calyx
by
fluoroscopy.
After
that,
guidewire
is
sent
into
the
kidney.
Thus
nephrostomy
tract
is
dilated
till
24F,
and
then
Amplatz
(24F)
is
sent
into
the
kidney,
and
then
nephroscopy
was
done
(wolf
17F).Next
lithotripsy
was
done
by
Swiss
pneumatic
lithoclast
and
stone
fragments
taken
out
from
the
kidney
after
checking
for
residual
stones
(by
fluoroscopy),
Nephrostomy
(16F)
was
inserted
and
fixed
and
the
operation
was
completed.
If
the
operation
was
prolonged
for
prevention
of
hyponatremia,
at
the
end
Lasix
(0.5
mg/kg)
was
prescribed.
Because
of
using
normal
saline
during
the
operation
for
irrigation,
dilutional
hyponatremia
is
produced,
thus
we
check
Na
&
K
after
the
operation.
Regarding
the
determined
special
objects,
the
results
of
the
study
are
the
following:
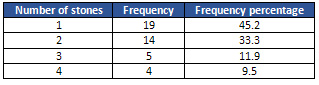
1.
Number
of
stones:
determining
the
number
of
stones
in
the
kidney
after
PNCL
operation
in
the
children
below
12
years
old
at
Jahrom
Paymanieh
hospital’s
urology
clinic,
during
2010-2014.
Though
the
study
was
been
done
on
43
patients,
the
number
of
existent
stones
in
42
patients
had
been
recorded.
Among
these
people
44.2
percent
of
them
had
one
stone
and
33.6
percent
had
two.
stones
and
11.9
percent
had
three
and
9.5
percent
had
4.
(Table
1,
Figure
1)
Table
1:
Frequency
percent
of
number
of
stones
Figure
1:
Frequency
percent
of
number
of
stones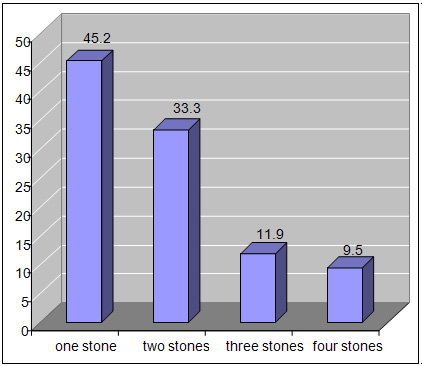
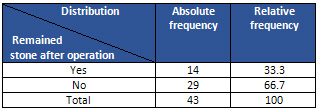
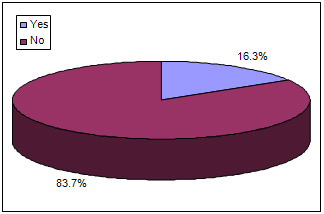
2.
Residual
stones:
To
determine
the
amount
of
remained
stone
after
operation
that
was
done
in
Jahrom
Paymanieh
hospital’s
urology
clinic,
during
2010-2014.
The
stones
were
completely
taken
out
from
the
kidney
of
43
patients
(85
percent
of
the
population)
and
their
operation
was
done
successfully.
Table
2:
Remained
stones
after
operation
Figure
2:
Relative
Frequency
of
Residual
stones
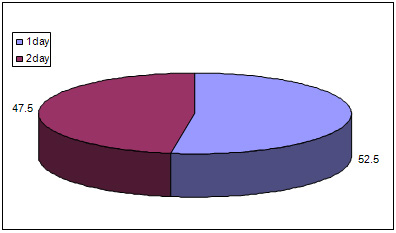
3.
Hospital
stay:
determining
the
average
time
of
hospitalization
for
children
below
12
years
old
who
were
suffering
from
renal
stone
after
PNCL
operation
at
Jahrom
Paymanieh
hospital’s
urology
clinic,
during
2010-2014.
The
average
time
of
hospitalization
was
31.11±12.59
hours.
The
longest
time
was
24
and
48
hours
that
respectively
included
33.3
and
26.2
percent.
Table
3:
Hospital
stay
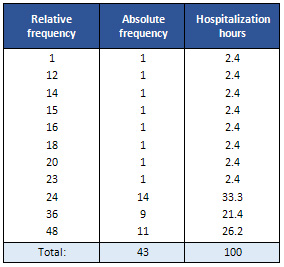
Figure
3:
Valid
percent
of
hospitalization
(days)
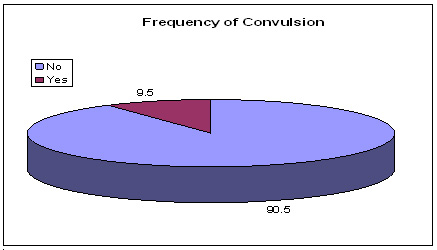
4.
Side
effects:
To
determine
the
PNCL
operation’s
side
effects
in
children
below
12
years
old
at
Jahrom
Paymanieh
hospital’s
urology
clinic,
during
2010-2014.
The
PNCL
operation’s
side
effects
were
recorded
for
42
of
patients,
infour
patients
this
involved
convulsion
and
38
patients
had
no
problems.
Table
4:
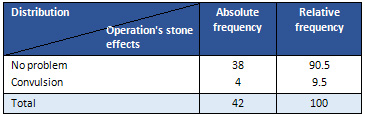
Figure
4
Pediatric
urolithiasis
poses
management
challenges
because
of
small
kidney
size,
less
knowledge
about
the
long-term
effects
of
newer
modalities
of
treatment
on
kidneys
and
etiology
of
the
stone.
Shock
wave
lithotripsy
is
the
treatment
of
choice
for
most
small
calculi,
while
PCNL
or
open
surgery
is
reserved
for
larger
stones
or
stones
with
anatomic
abnormalities.Aim
of
treatment
is
complete
clearance
and
treatment
of
the
underlying
cause.
The
first
series
on
pediatric
PCNL
was
published
by
Woodside
et
al
claiming
a100%
stone
free
rate
with
no
significant
complications.
They
used
standard
dilatation
technique.
In
series
reported
by
Boddy
et
al”
90%
stone
free
rate
was
achieved
and
after
sequential
dilatation
24
to
26
F
sheath
was
used
with
no
major
complications.
Segura
has
suggested
the
use
of
adult
instruments
in
children.
Desai
et
al
(17),suggests
limited
tract
dilatation
<
21
F
and
use
of
pediatric
instruments.
The
drawback
with
pediatric
instruments
is
small
instrument
port,
which
necessitates
use
of
small
probes
and
forceps.
This
results
in
prolongation
of
operation
time.
Blood
loss
is
a
major
complication
of
pediatric
PCNL,
which
is
directly
related
to
tract
size
dilatation.
Reduced
incidence
of
major
intra
renal
vessel
injury
using
a
pediatric
nephroscope
has
been
reported
by
Zanetti
et
al(6).
It
is
believed
that
adult
instruments
may
cause
more
bleeding
and
amplatz
may
be
too
big
for
the
pediatric
kidneys.
We
have
been
doing
PCNL
on
pediatric
patients
since
1988
using
adult
instruments
(Stortz)
without
any
significant
problem.
Since
1994
this
problem
was
taken
care
of
in
our
series
by
using
Wolf
adult
nephroscope
inner
sheath
(20
F),
which
allowed
placement
of
smaller
amplatz
sheath(2).
More
effective
fragmentation
of
stone
was
achieved
using
adult
size
ultrasonic
and
pneumatic
energy
sources.
The
advantages
of
this
technique
are
better
visibility,
quick,
effective
stone
fragmentation
and
retrieval
using
adult
size
energy
probes
and
stone
graspers.
One
can
avoid
buying
a
separate
pediatric
set
of
instruments
which
may
result
in
considerable
cost
saving
for
a
department
in
a
developing
country.
Since
the
advent
of
PCNL
in
1976,
the
techniques
have
been
greatly
improved.
Many
medical
centers
have
used
adult-sized
nephroscopes
in
children(11).
But
percutaneous
stone
therapy-related
hemorrhage
requires
a
blood
transfusion
(11%-14%),
and
an
increased
risk
of
kidney
loss.
Therefore,
conventional
percutaneous
nephrolithotomy
is
not
justified
as
the
primary
form
of
urinary
stone
treatment
for
smaller
lower
pole
concernments,
although
it
is
recommended
as
an
effective
method
in
children.
Percutaneous
nephrolithotomy
using
ureter
scope
and
pneumatic
intra
corporeal
lithotripsy
in
children
was
introduced
to
our
hospital
in
2002(18).
In
this
study,
the
stones
were
removed
completely
with
minimal
injury
to
renal
tissue,
while
retrieving
large
fragments
quickly.
The
duration
of
the
procedure
was
75
minutes.
The
level
of
hemoglobin
decreased
by
14
g/L
on
average.
None
of
the
patients
received
blood
transfusion.
To
date,
there
has
been
only
one
recurrence
of
stone
and
no
other
complications
have
occurred.
Traditional
percutaneous
nephrolithotomy
uses
a
30-Fr
nephrostomy
sheath
for
renal
access.
In
order
to
reduce
blood
loss
and
absorption
of
irrigant,
stone
extraction
may
be
performed
when
the
established
access
tracts
become
mature.
The
recent
development
of
smaller
sheaths
suggests
that
percutaneous
nephrostomy
tract
formation
can
be
performed
with
minimal
injury
to
the
involved
renal
parenchyma,
thereby
reducing
the
procedure-related
morbidity.
We
used
ureter
scope
and
pneumatic
intra
corporeal
lithotripsy
in
pediatric
patients.
The
operating
tract
was
small
(12F-18F),
therefore
only
2
operations
were
discontinued
because
of
greater
blood
loss
in
the
process
of
dilatation,
but
the
second
operations
were
successful.
During
PCNL,
the
common
mistake
especially
for
stag
horn
in
children
is
overdoing
through
a
single
tract,
even
when
another
tract
is
needed.
Torqueing
a
rigid
ureter
scope
against
the
pelvi-caliceal
system
to
get
to
an
inaccessible
calix
is
the
most
important
cause
of
bleeding
during
PCNL
and
is
largely
responsible
for
the
increased
rates
of
transfusion
and
extravasation.
We
believe
that
judiciously
making
multiple
tracts
does
not
significantly
increase
intraoperative
complications
and
transfusion.
Using
multiple
tracts
when
necessary
avoids
the
excessive
use
of
torque
to
gain
entry
into
adjacent
calices,
which
may
cause
infundibula
tear
and
bleeding.
In
the
present
series,
multiple
tracts
were
used
in
8
kidneys.
As
a
result,
better
and
faster
clearance
of
large-volume
stag
horn
calculi
was
achieved
without
significant
increase
in
morbidity.
PCNL
has
a
better
stone
clearance
rate
and
is
cost-effective.
It
is
characterized
by
convalescence
compared
with
other
modalities
such
as
ESWL
and
open
surgeries
for
removal
of
the
stones.
In
our
series,
PCNL
achieved
a
complete-clearance
rate
of
91%,
and
an
overall
clearance
rate
of
100%
when
it
was
combined
with
ESWL.
In
children
with
large
renal
stones
(>3
cm),
stag
horn
calculi
(complete
and
partial),
complex
or
multiple
calculi,
renal
insufficiency,
recurrent
stones,
and
stones
refractory
to
ESWL,
PCNL
is
considered
the
treatment
of
choice.
The
use
of
a
less
traumatic
18-Fr
access
sheath
is
effective
in
children
with
large
renal
stones.
A
prerequisite
for
stone
clearance
is
the
establishment
of
optimal
access
to
the
collecting
system
of
the
kidney.
Staging
the
procedure
in
selecting
patients
is
very
important
to
reduce
the
caliber
of
the
percutaneous
tract
in
children
with
non-dilated
collecting
system
(19).
| | |
