|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
........................................................
|
|
Original contribution/Clinical Investigation
Diabetes Mellitus
- Knowledge, Management and Complications: Survey
report from Faisalabad-Pakistan
Ijaz Anwer, Ahmad Shahzad, Kashmira Nanji, Farah
Haider, Muhammad Masood Ahmad
Alanine aminotransferase
indicates excess weight and dyslipidemia
Mehmet Rami Helvaci, Orhan Ayyildiz* Mustafa
Cem Algin, Yusuf Aydin, Abdulrazak Abyad, Lesley
Pocock
Comparative Analysis of Antimicrobial Peptides
Gene Expression in Susceptible/Resistant Mice
Macrophages to Leishmania major Infection
Hamid Daneshvar, Iraj Sharifi, Alireza Kyhani,
Amir Tavakoli Kareshk, Arash Asadi
Does
socio-economic status of the patients have effect
on clinical outcomes after coronary artery bypass
grafting surgery?
Forough Razmjooei, Afshin Mansourian, Saeed
Kouhpyma
Comparison of the uterine
artery Doppler indices during pregnancy between
gestational diabetes and diabetes mellitus and
healthy pregnant women
Nazanin Farshchian, Farhad Naleini, Amir Masoud
Jaafarnejhad,
Parisa Bahrami Kamangar
Survey single dose
Gentamicin in treatment of UTI in children with
range of 1 month to 13 years old in Jahrom during
2015
Ehsan Rahmanian, Farideh Mogharab,
Vahid Mogharab
Evaluation of control of
bleeding by electro cauterization of bleeding
points of amplatz sheath tract after percutaneous
nephrolithotomy (PCNL) in Jahrom Peymanieh hospital
during year 2015-2016
Ali Reza Yousefi , Reza Inaloo
Comparison of the three-finger
tracheal palpation technique with triple ID
formula to determine endotracheal tube depth
in children 2-8 years in 2016-2017
Anahid Maleki, Alireza Ebrahim Soltani, Alireza
Takzare, Ebrahim Espahbodi,
Mehrdad Goodarzi , Roya Noori
Effect of Sevoflurane
and Propofol on pulmonary arterial pressure
during cardiac catheterization in children with
congenital heart diseases
Faranak Behnaz, Mahshid Ghasemi , Gholamreza
Mohseni, Azim Zaraki
Population and Community Studies
Prevalence
and risk factors of obesity in children aged
2-12 years in the Abu Dhabi Islands
Eideh Al-Shehhi, Hessa Al-Dhefairi, Kholoud
Abuasi, Noora Al Ali, Mona Al Tunaiji, Ebtihal
Darwish
Study and comparison
of psychological disorders in normal students
and students with multiple sclerosis in Shahrekord
Neda Ardestani-Samani, Mohammad Rabiei, Mohammad
Ghasemi-Pirbalooti, Asghar Bayati, Saeid Heidari-Soureshjani
Comparative
study of self-concept, physical self-concept,
and time perspective between the students with
multiple sclerosis and healthy students in Shahrekord
Neda Ardestani-Samani, Mohammad Rabiei, Mohammad
Ghasemi-Pirbalooti, Asghar Bayati, Saeid Heidari-Soureshjani
Relationship
between Coping Styles and Religious Orientation
with Mental Health in the Students of the Nursing-Midwifery
Faculty of Zabol
Nasim Dastras, Mohsen Heidari Mokarrar, Majid
Dastras, Shirzad Arianmehr
Tuberculosis in Abadan,
Iran (2012-2016): An Epidemiological Study
Ali-Asghar ValiPour, Azimeh Karimyan, Mahmood
Banarimehr, Marzieh Ghassemi, Maryam Robeyhavi,
Rahil Hojjati,
Parvin Gholizadeh
Family Stability and Conflict
of Spiritual Beliefs and Superstitions among
Yazdi People in Iran: A Qualitative Study
Zahra Pourmovahed , Seyed Saied Mazloomy Mahmoodabad
; Hassan Zareei Mahmoodabadi ; Hossein Tavangar
; Seyed Mojtaba Yassini Ardekani ; Ali Akbar
Vaezi
A comparative
study of the self-actualization in psychology
and Islam
Simin Afrasibi, Zakieh Fattahi
The effectiveness
of cognitive - behavioral therapy in reducing
the post-traumatic stress symptoms in male students
survivors of earthquake in the central district
of Varzeghan
Sakineh Salamat, Dr.Ahad Ahangar, Robab Farajzadeh
Reviews
Effects and mechanisms
of medicinal plants on stress hormone (cortisol):
A systematic review
Kamal Solati, Saeid Heidari-Soureshjani, Lesley
Pocock
Comparing Traditional
and medical treatments for constipation : A
Review Article
Mohammad Yaqub Rajput
A review of anti-measles
and anti-rubella antibodies in 15- 25 year old
women in Jahrom City in 2011
Ehsan Rahmania , Farideh Mogharab, Vahid Mogharab
Review of percutaneous
nephrolithotomy in children below 12 years old
in Jahrom hospital, during 2010-2014
Ali Reza Yousefi , Reza Inaloo
Physical and
mental health in Islam
Bahador Mehraki, Abdollah Gholami
International Health Affairs
The Challenges of Implementation
of Professional Ethics Standards in Clinical Care
from the viewpoint of Nursing Students and Nurses
Saeedeh Elhami, Kambiz Saberi, Maryam Ban, Sajedeh
Mousaviasl, Nasim Hatefi Moadab, Marzieh Ghassemi
Cognitive Determinants
of Physical Activity Intention among Iranian Nurses:
An Application of Integrative Model of Behavior
Prediction
Arsalan Ghaderi, Firoozeh Mostafavi, Behzad Mahaki,
Abdorrahim Afkhamzadeh,
Yadolah Zarezadeh , Erfan Sadeghi
Effect of resilience-based
intervention on occupational stress among nurses
Hossein Jafarizadeh, Ebrahim Zhiyani, Nader
Aghakhani, Vahid Alinejad, Yaser Moradi
Education and Training
Calculation of Salaries
and Benefits of Faculty Members in the Ministry
of Health and Medical Education of Iran
Abdolreza Gilavand
The effect of education
on self-care behaviors of gastrointestinal side
effects on patients undergoing chemotherapy
Shokoh Varaei, Ehsan Abadi Pishe, Shadan Pedram
Razie, Lila Nezam Abadi Farahani
Creating and
Validating the Faith Inventory for Students
at Islamic Azad University of Ahvaz
Solmaz Choheili, Reza Pasha, Gholam Hossein
Maktabi, Ehsan Moheb
Creating
and Validating the Adjustment Inventory for
the Students of Islamic Azad University of Ahvaz
Homa Choheili, Reza Pasha, Gholam Hossein Maktabi,
Ehsan Moheb
Evaluating
the Quality of Educational Services from the
Viewpoints of Radiology Students of Ahvaz Jundishapur
University of Medical Sciences
Abdolreza Gilavand, Jafar Fatahiasl
An Investigation
of Psychosocial aspect of Iranian Nursing Students'
Clinical Setting
Mahsa Boozaripour , Zanyar Karimi, Sima Zohari
Anbohi, Amir Almasi-Hashiani, Fariba Borhani
Clinical Research and Methods
Comparison of the
Antibacterial Effects of Chlorhexidine Mouth
washes with Jaftex Mouth wash on Some Common
Oral Microorganisms (An in Vitro Study)
Ebrahim Babadi, Zahra Bamzadeh, Fatemeh Babadi
Study of the effect
of plasma jet on Fusarium isolates with ability
to produce DON toxins
Elham Galin Abbasian, Mansour Bayat, Arash chaichi
Nosrati, Seyed Jamal Hashemi, Mahmood Ghoranneviss
The comparison of
anti-inflammatory effect in two methods of topical
dexamethasone injection and topical application
of ginger alcoholic extract after removing mandibular
wisdom teeth
Sahar Zandi, Seyyed Muhammadreza Alavi, Kamran
Mirzaie, Ramin Seyedian, Narges Aria, Saman
Jokar
The effect of curcumin
on growth and adherence of major microorganisms
causing tooth decay
Leila Helalat, Ahmad Zarejavid, Alireza Ekrami,
Mohammd Hosein Haghighizadeh, Mehdi Shiri Nasab
|
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| November 2017
- Volume 15, Issue 9 |
|
|
Prevalence and risk factors
of obesity in children aged 2–12 years
in the Abu Dhabi Islands
Eideh Al-Shehhi (1)
Hessa Al-Dhefairi (1)
Kholoud Abuasi (1)
Noora Al Ali (1)
Mona Al Tunaiji (2)
Ebtihal Darwish (2)
(1) Family Medicine Residents
(2) Supervisors
Corresponding author:
Eideh Al-Shehhi
Family Medicine Resident
Family Medicine Residency Program
Sheikh Khalifa Medical City
Email: ealshehhi@seha.ae
|
Abstract
Background: The
prevalence of childhood obesity has grown
at an alarming rate worldwide over the
last few decades. The negative health
outcomes of obesity, including the increased
risk of non-communicable disease, morbidity,
mortality, and the cost of health services,
make this condition a major public health
problem.
Aim: To
measure the prevalence and risk factors
of obesity in children aged 2–12
years in the Abu Dhabi Islands, United
Arab Emirates.
Methods: A
questionnaire was submitted to 274 mothers
with children aged 2–12 years at
2 governmental ambulatory health care
centers in Abu Dhabi. This cross-sectional
study was conducted between February 2014
and January 2015.
Results:
The prevalence of overweight and obesity
among the study population was found to
be 32.8% overall (15.3% and 17.5%, respectively).
In the study population, 59.1% were of
normal weight and 8% were underweight.
The prevalence of childhood obesity was
found to be higher among UAE nationals
than non-UAE-nationals (22.2% vs. 10.4%;
p = 0.016). We observed a statistically
significant relationship between obesity
and child age (p = 0.001), with 6.2% of
children aged 2–4 years being obese
compared to 29.2% of children aged 11–12
years. Parents of the obese children underestimated
the problem. We found that in 84% of normal
weight children, their parents perceived
them as having a normal weight. By comparison,
only 16% of obese children were perceived
by their parents as obese. This difference
is statistically significant (p < 0.001).
Conclusion:
The prevalence of overweight and obesity
among children is increasing in the UAE,
especially among UAE nationals. Moreover,
obesity increases with age, and children
who are obese in the first years of their
life will stay obese in their late childhood.
Most parents of obese children fail to
perceive their children as obese.
Key words: obesity,
children, Abu Dhabi
|
The prevalence of obesity is rapidly growing
worldwide. The World Health Organization estimates
that 42 million children under the age of five
are obese (WHO, 2015). Based on available data,
overweight and obese children are more likely
to remain obese into adulthood. With the increased
incidence of obesity in children, more health
problems are expected in the next generation
of adults. Cardiovascular diseases, diabetes,
joint diseases, endocrine disorders, respiratory
problems, several types of cancer, psychological
stresses, and other obesity-related conditions
will be found in the next young adult populations.
The negative impact of obesity on morbidity,
mortality, and healthcare costs make this condition
a major public health problem.
High rates of childhood overweight have been
reported in many developing countries, including
the Middle Eastern countries. The UAE is one
of the developing countries that has gone through
a rapid socioeconomic transition over the past
four decades, leading to fundamental changes
in the population’s lifestyle, dietary
habits, and physical activities.
A genetic predisposition is a significant risk
factor for childhood obesity and overweight,
but the global rise in the prevalence of childhood
obesity suggests that factors other than genes
are involved. Changes in the world food economy
and the trend toward a sedentary lifestyle are
considered the main reasons for this public
health problem (T. Lobstein, 2004). Increased
energy-dense diets that are high in fat, particularly
saturated fat, and low in unrefined carbohydrates,
in addition to motorized transport, labor saving
devices at home, and physically undemanding
leisure activities are examples of obesity risk
factors today.
Many people believe that dealing with overweight
and obesity is a personal responsibility. To
some degree they are right, but it is also a
community responsibility. The community has
a responsibility to provide safe, accessible
places for children to play or ride a bike.
Schools should have daily physical education
and provide healthy food choices. Mothers should
be educated by their doctors about the benefits
of breast-feeding and how to prevent childhood
obesity. All these measures are examples of
how the community can assume some responsibility
in addressing the problem of childhood obesity.
For children aged 2–19 years, the WHO
defines overweight as a BMI at or above the
85th percentile and lower than the 95th percentile
and obesity as a BMI at or above the 95th percentile
for children of the same age and sex. The calculated
BMI can be plotted on a BMI-for-age growth chart
to obtain a percentile ranking. These percentiles
are the most commonly used indicators for assessing
the size and growth patterns of individual children
(WHO, 2015). This study aims to determine the
prevalence and risk factors for obesity in children
aged 2–12 years in the Abu Dhabi Islands,
UAE.
The percentage of children aged 6–11 years
in the United States who were obese increased
from 7% in 1980 to nearly 18% in 2012. Similarly,
the percentage of adolescents aged 12–19
years who were obese increased from 5% to nearly
21% over the same period (CDC, 2015). In 2012,
more than one-third of children and adolescents
in the US were overweight or obese (CDC, 2015).
Significant changes in UAE society over the
last 30 years have brought about profound increases
in the number of overweight individuals (Al-Hourani
HM, 2003). The prevalence of childhood obesity
in the UAE is surpassing the international standards
of obesity among children and adolescents (A.A.
Bin Zaal, 2011). A sample of UAE school children
found 1.8 times more obese children than in
the US (Al-Haddad FH, 2000). In the year 2000,
obesity and overweight among UAE children was
estimated at 8.3% using data from a UAE National
Survey of school-aged individuals (Cole TJ,
2000). Another study published in 2012 specifically
in the Emirate of Abu Dhabi showed that 14.7%
of school-aged children are overweight and 18.9%
are obese. Further analysis restricted to UAE
nationals showed that 14.2% were overweight
and 19.8% were obese (A Al Junaibi, 2012).
Comparing the UAE to other Gulf countries,
the prevalence of overweight was found to be
nearly 2–3 times higher in both sexes compared
to their Bahraini counterparts; compared to
their Kuwaiti counterparts aged 12–14 years,
the prevalence of obesity amongst Dubai adolescents
was 1.5–2 times higher (A.A. Bin Zaal,
2011).
Overweight children are at increased risk of
being obese in adolescence. A study conducted
by Al Haddad in 2005 showed that overweight
UAE males increased in frequency from 16.4%
at age 10 to more than 29% at age 18, and obesity
increased from 6.1% at age 10 to 18% at age
18. UAE female children exhibited a different
pattern: 22.8% were overweight at age 10 years,
and more than 27% were overweight at 18 years.
Obesity among UAE females increased from 7.8%
at 10 years of age to 9.6% at 18 years of age
(Al-Haddad FH, 2005).
Al Junaibi identified several independent determinants
of obesity, including older age, male sex, lack
of dairy consumption, and higher parental BMI.
The same study showed no associations with exercise,
perhaps due to the inaccurate self-reported
nature of this variable (A Al Junaibi, 2012).
Another study by Al-Junaibi found that 33.8%
of the parents of overweight/obese children
misclassified their child’s weight status,
either by underestimation (27.4%) or overestimation
(6.3%). Misclassification was highest among
parents of overweight/obese children (63.5%)
and underweight (55.1%) children (Abdulla Aljunaibi,
2013).
Multiple factors underlie childhood obesity,
including diet and lack of exercise. Nepper
and Chai showed that 40% of the food consumed
by children and adolescents is high in calories
and fat, including sugar-sweetened beverages,
junk food, and desserts. In a study in which
students, parents, and teachers were interviewed,
all subjects confirmed that there are barriers
to accessing healthy foods in the school and
community (Kelly Stott, 2012).
A study of children in the UAE cited cultural
and weather restrictions as the main reasons
for their lack of physical activity (Al-Hourani
HM, 2003). The study found that although there
was less watching of television on school days
(less than 2 hours a day) compared to weekends
(3 hours), there was no significant difference
in energy expenditure between school days and
weekends. Al-Hourani attributed this observation
to the high temperatures during daylight hours.
In addition, Al-Hourani stated that female children
find it difficult to wear clothes suitable for
exercise, which may impede their interest in
physical activity (Al-Hourani HM, 2003). As
children grow older, they tend to spend less
time sleeping and more time doing physical activities.
However, the same study found that this general
trend is not true for adolescent females living
in the UAE, as the time spent sleeping and engaging
in physical activity were similar between girls
aged 11–13 years and 14–16 years.
In fact, the number of hours spent sleeping
was high in both groups (Al-Hourani HM, 2003)
Study
design
This
cross-sectional,
questionnaire-based
study
was
conducted
at
2
randomly-chosen
ambulatory
health
care
centers
on
the
Abu
Dhabi
Islands:
the
Al
Bateen
clinic
and
the
Zaafarana
clinic.
Study
participants
Children
aged
2–12
years
(n
=
274)
and
their
parents
were
recruited
from
February
2014
to
January
2015.
Children
with
chronic
diseases,
children
of
parents
who
were
non-Arabic
and
non-English
speakers,
and
children
not
accompanied
by
their
parents
were
excluded
from
the
study.
The
total
study
population
size
was
estimated
to
be
1,253
based
on
clinic
visits
the
same
months
of
the
previous
year.
The
sample
size
of
291
was
calculated
using
a
sample
size
calculator
with
95%
CI
and
5%
margin
of
error.
The
final
sample
size
was
274
after
the
exclusion
of
17
subjects
because
of
missing
medical
records.
Questionnaire
The
questionnaire
was
developed
based
on
those
used
in
previously
reported
studies.
The
questionnaire
was
divided
into
three
parts:
1)
Questions
regarding
family
socio-demographic
factors
and
parental
factors
contributing
to
the
development
of
childhood
obesity
(8
questions);
2)
Questions
regarding
the
child’s
lifestyle,
including
dietary
practices,
physical
activities,
and
sleeping
hours
(11
questions);
3)
Questions
regarding
physical
parameters,
including
the
child’s
weight,
height,
and
BMI.
The
questionnaire
was
prepared
in
2
versions,
Arabic
and
English.
Part
1
of
the
questionnaire
included
the
ages
of
the
parents
(20–30
years,
31–40
years,
41–50
years,
or
above
50
years),
nationality
(UAE
national
or
non-UAE
national),
level
of
education
(illiterate,
primary
school,
secondary
school,
or
university),
family
income
(very
low,
not
sufficient,
sufficient,
more
than
sufficient),
whether
either
parent
was
overweight
or
obese
(yes
or
no),
the
number
of
children
in
the
family
(1–2,
3–4,
5–6,
or
more
than
7),
and
age
of
the
child
subject
(2–4,
5–7,
8–10,
or
11–12
years).
Part
2
included
questions
regarding
the
consumption
of
healthy
food
and
junk
food
(never,
rare,
sometimes,
or
always),
activities
including
watching
TV,
video
games,
iPad
use
(never,
1–3,
4–6,
or
more
than
6
h),
exercise
(never,
1–2,
3–4,
or
5
or
more
times/week),
and
sleeping
hours
(less
than
4,
4–6,
7–10,
or
more
than
10
hours/day),
and
parent’s
impression
of
their
child’s
weight
(thin,
normal,
overweight,
or
obese).
Part
3
asked
about
the
child’s
weight
(kg),
height
(cm),
and
BMI
(number
and
percentile).
A
pilot
study
was
conducted
before
finalizing
the
questionnaire,
and
modifications
were
made
accordingly.
Data
collection
All
children
aged
2–12
years
who
were
accompanied
by
a
parent,
were
approached
by
a
staff
nurse
to
request
their
participation
in
the
study
until
the
sample
size
was
achieved.
The
BMIs
were
obtained
from
the
medical
records
of
all
selected
participants.
Trained,
qualified
nurses
working
in
the
ambulatory
health
service
assessed
the
growth
characteristics
of
the
children
as
part
of
routine
health
care
at
each
clinic
visit.
They
measured
the
height
and
weight
using
an
electronic
scale
and
height
meter.
The
height
was
measured
with
the
subject
in
a
standing
position
without
shoes,
and
the
weight
was
measured
while
the
subject
wore
light
clothing.
Growth
charts
and
parameters,
including
BMIs,
were
recorded
by
the
nurses
using
a
computerized
system.
Statistical
analysis
The
data
were
organized
using
the
Excel
software
program
and
analyzed
using
the
Statistical
Package
for
Social
Sciences
(SPSS)
version
18.
The
total
and
sub-category
scores
were
compared
with
each
other
and
with
socio-demographic
factors
using
the
Pearson
correlation
coefficient
(r)
and
chi-square
coefficient
(2).
A
p-value
<0.05
was
considered
indicative
of
statistical
significance.
Ethics
approval
The
National
Institute
of
Health
(NIH)
web-based
training
course
“Protecting
Human
Research
Participants,”
was
completed
to
meet
the
ethics
requirements.
Approval
was
obtained
from
the
SKMC
Institutional
Review
Board/Research
Ethics
Committee
(IRB/REC)
in
February
2014.
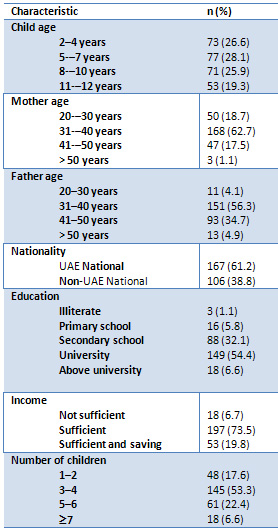
Demographic
characteristics
of
participants
This
study
enrolled
274
participants,
71.9%
of
whom
were
accompanied
by
their
mothers
and
28.1%
by
their
fathers.
The
majority
of
the
parent
participants
were
31–40
years
old
(62.7%
of
mothers,
56.3%
of
fathers).
The
cohort
comprised
61.2%
UAE
nationals
and
38.8%
non-UAE-nationals.
The
majority
of
the
respondents
(54.4%)
were
university
graduates,
while
1.1%
were
illiterate.
The
perceived
family
income
was
sufficient
in
73.5%,
sufficient
with
savings
in
19.8%,
and
insufficient
in
6.7%.
Most
of
the
participants
had
3–4
children
(53.3%),
while
17.6%
had
1–2,
22.4%
had
5–6,
and
only
6.6%
had
7
or
more.
The
age
distribution
of
the
child
participants
was
almost
uniform,
with
26.6%
age
2–4,
28.1%
5–7,
25.9%
8–10,
and
19.3%
11–12
years.
The
socio-demographics
of
the
study
population
are
presented
in
Table
1.
Table
1.
Socio-demographic
data
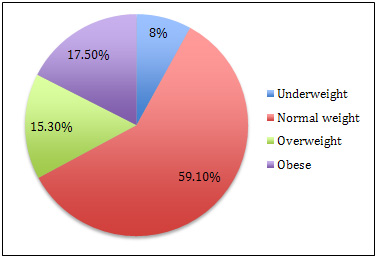
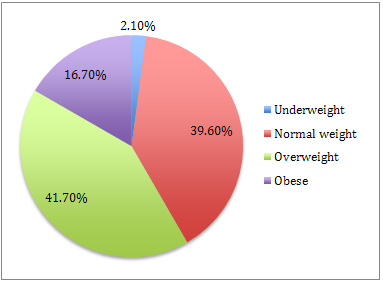
Prevalence
of
overweight
and
obesity
The
prevalence
of
overweight
and
obesity
in
the
study
population
was
found
to
be
32.8%
(15.3%
and
17.5%,
respectively),
with
59.1%
of
normal
weight
and
8%
underweight
(Figure
1).
Figure
1.
Prevalence
of
childhood
obesity
(2–12-year-olds)
in
the
Abu
Dhabi
Islands
(n
=
274)
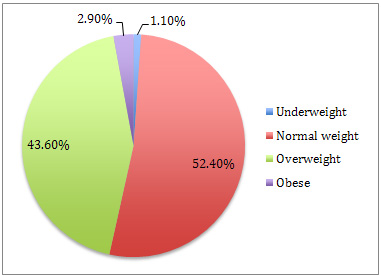
Parent
perception
of
weight
When
asked
about
their
own
weight,
52.4
%
of
the
parents
perceived
themselves
as
normal
weight,
while
43.6%
saw
themselves
as
overweight
and
2.9%
saw
themselves
as
obese
(Figure
2).
Figure
2.
Parent
perception
of
their
own
weight
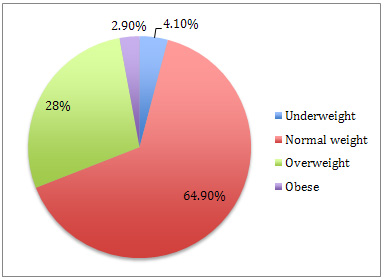
When
asked
about
their
spouse’s
weight,
4.1%
of
the
parents
perceived
their
spouse
as
underweight,
64.9%
as
normal,
28%
as
overweight,
and
3%
as
obese
(Figure
3).
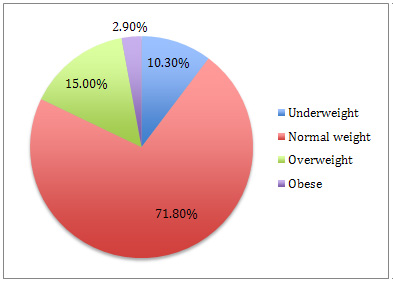
The
majority
of
the
respondents
perceived
their
child’s
weight
as
normal
(71.8%),
while
only
15%
perceived
their
children
as
overweight
and
2.9%
as
obese
(Figure
4).
Figure
3:
Parent
perception
of
spouse’s
weight
Figure
4:
Parent
perception
of
child’s
weight
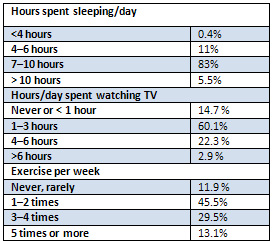
Child
lifestyle
Of
the
child
participants,
0.4
%
slept
less
than
4
hours/day,
11%
slept
4–6
hours/day,
83%
slept
7–10
hours/day,
and
5.5
%
slept
more
than
10
hours/day.
The
majority
of
children
spent
1–3
hours/day
watching
TV
(60.1%),
while
a
minority
(2.9%)
watched
TV
for
more
than
6
hours/day.
Most
of
the
children
exercised
1–2
times/week
(45.5%),
while
only
11.9%
exercised
rarely
or
never
(Table
2).
Table
2:
Child
lifestyle
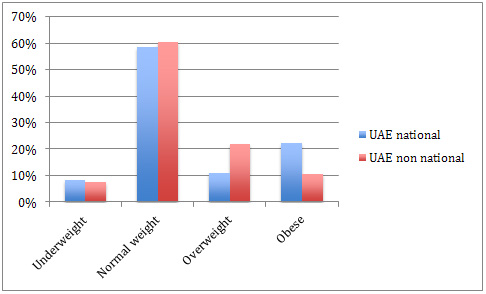
The
prevalence
of
childhood
obesity
was
found
to
be
higher
among
UAE
nationals
than
non–UAE-nationals
(22.2%
vs.
10.4%;
p
=
0.016)
(Figure
5).
Figure
5.
Obesity
prevalence
among
UAE
nationals
vs.
non-nationals
(n
=
274)
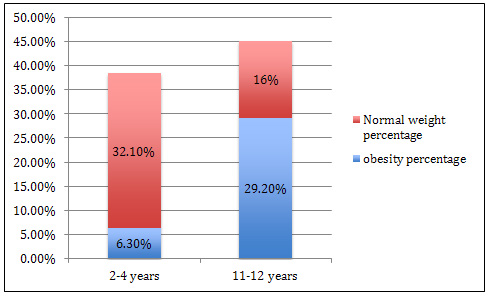
Obesity
and
child
age
correlated
significantly
(p
=
0.001),
with
obesity
in
6.2%
of
children
aged
2–4
years
compared
to
33.3%
of
children
aged
8–10
years
(Figure
6).
The
parents
of
84%
of
normal
weight
children
perceived
their
child
as
having
a
normal
weight,
while
16%
of
the
parents
of
obese
children
perceived
their
child
as
obese.
This
finding
was
statistically
significant
(p
<
0.001)
(Figure
7).
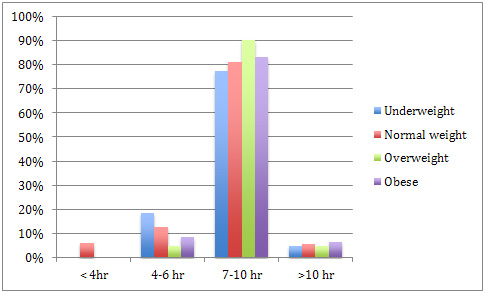
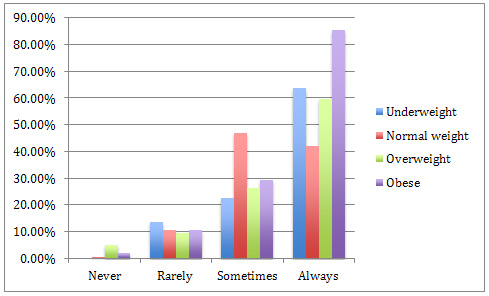
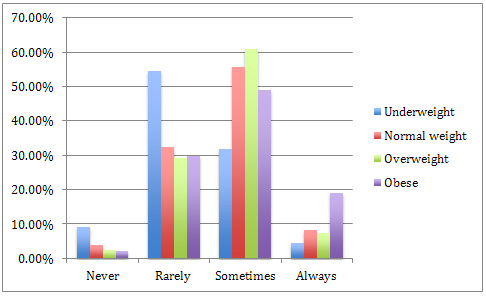
Most
of
the
children
slept
7–10
hours,
regardless
of
their
weight
(normal
weight,
81%
of
participants;
overweight,
90%;
obese,
85.4%)
(Figure
8).
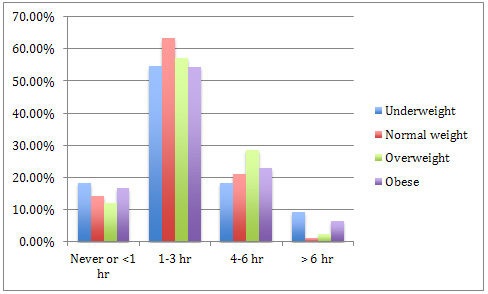
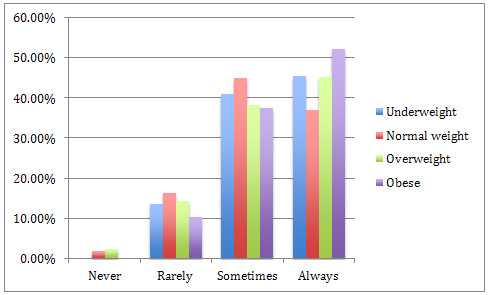
The
majority
of
children
spent
1–3
hours/day
watching
TV
(normal
weight,
63%;
obese,
54.2%)
(Figure
9).
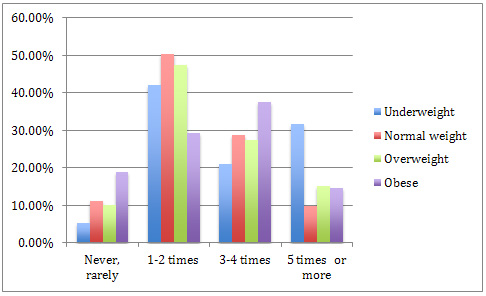
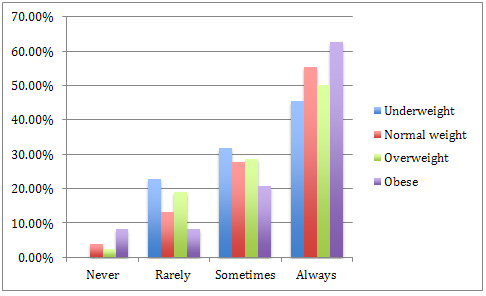
Most
of
the
obese
children
exercised
3–4
times/week
(37.5%),
while
the
majority
of
overweight
and
normal
weight
children
exercised
1–2
times
per
week
(47.5%
and
50%,
respectively)
(Figure
10).
Figure
6:
Association
between
child
age
and
obesity
Figure
7:
Parent
perception
of
their
obese
child’s
weight
status
Figure
8:
Association
between
hours
slept/day
and
child
weight
Figure
9:
Association
between
hours/day
spent
watching
TV
and
child
weight
Figure
10.
Association
between
exercise
hours/week
and
child
weight
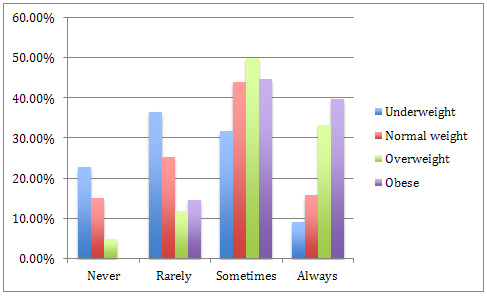
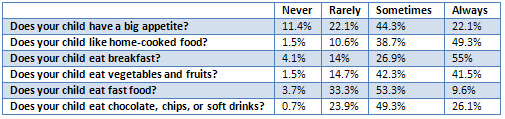
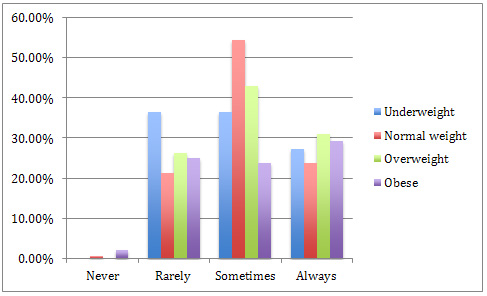
Eating
habits
Most
children
reported
a
good
appetite
(44.3%),
while
11.4%
reported
never
having
a
good
appetite.
Of
the
obese
children,
39%
always
had
good
appetite
compared
to
only
15.7%
of
normal
weight
and
9.1%
of
underweight
children.
This
difference
is
statistically
significant
(p
<
0.001)
(Figure
11).
The
majority
of
children
always
ate
home-cooked
food
(49.3%),
while
only
1.5%
never
ate
home-cooked
food.
The
majority
of
children
(55%)
always
ate
breakfast,
while
a
minority
(4.1%)
never
did.
Fruits
and
vegetables
were
sometimes
eaten
by
42.3%
of
the
children
and
never
eaten
by
1.5%.
The
majority
of
obese
children
always
ate
home-cooked
food,
breakfast,
and
vegetables
and
fruits
(Figure
12,
13,
and
14,
respectively).
Fast
food
was
eaten
by
53.3%
of
the
children;
only
3.7
%
never
ate
fast
food.
Chocolate,
chips,
and
soft
drinks
were
sometimes
eaten
by
49.3%
of
the
children
and
never
eaten
by
0.7%
(Table
3)
The
majority
of
the
overweight
and
obese
children
sometimes
eat
these
foods
(Figures
15,
16,
respectively).
Figure
11:
Association
between
appetite
and
child
weight
Figure
12:
Association
between
eating
home-cooked
food
and
child
weight
Figure
13:
Association
between
eating
breakfast
and
child
weight
Figure
14.
Association
between
eating
vegetables
and
fruits
and
child
weight
Table
3:
Child
eating
habits
Figure
15.
Association
between
eating
fast
food
and
child
weight
Figure
16.
Association
between
eating
chocolate,
chips,
and
soft
drinks
and
child
weight
Our
results
show
that
the
prevalence
of
overweight
and
obesity
among
children
in
the
Abu
Dhabi
Islands
is
15.3%
and
17.5%,
respectively.
Similar
results
were
found
in
another
Abu
Dhabi
study
published
in
2012,
reporting
that
14.7%
of
children
were
overweight
and
18.9%
were
obese.
That
study
reported
that
obesity
among
UAE
nationals
was
19.8%
compared
to
22.2%
in
this
study,
conducted
3
years
later.
This
indicates
that
the
problem
is
increasing.
We
observed
a
statistically
significant
relationship
between
obesity
and
child
age
in
our
study
(p
=
0.001).
The
same
conclusion
was
reached
by
Al-Haddad,
as
discussed
in
the
literature
review.
A
similar
finding
was
seen
in
a
CDC
report
that
showed
the
prevalence
of
obesity
in
children
(6–12
years
old)
in
the
United
States
was
18%
in
2012,
indicating
that
obesity
is
a
global
public
health
issue.
Parental
participation
is
a
key
factor
in
the
prevention
and
management
of
childhood
obesity.
Parental
perception
of
their
children’s
weight
status
was
measured
in
our
study,
and
the
majority
of
parents
of
overweight/obese
children
(84%)
underestimated
their
child’s
weight
status.
In
2013,
Al-Junaibi
found
that
63%
of
parents
of
overweight/obese
children
underestimated
their
weight
and
perceived
their
child
as
having
a
normal
weight.
Previous
studies
have
shown
that
the
level
of
education,
income,
sedentary
lifestyle,
less
physical
activity,
and
a
tendency
toward
high-calorie
diets
are
factors
contributing
to
obesity.
These
factors
were
not
identified
as
significant
in
our
study,
limiting
our
ability
to
formulate
clear
intervention
guidelines.
However,
differences
between
our
study
and
other
studies,
including
methodology,
sample
selection,
sample
size,
and
design,
may
limit
their
comparability.
Our
findings
provide
a
warning
signal
that
obesity
in
children
has
become
a
major
health
problem
in
our
country
and
may
have
further
negative
consequences
in
the
future.
Further
research
is
needed
to
understand
the
underlying
causes
of
this
problem
and
to
devise
appropriate
recommendations
for
its
prevention.
The
questionnaire
used
in
this
study
was
not
validated,
which
may
be
a
limitation
of
this
study.
In
addition,
the
lack
of
previous
similar
research
limits
the
scope
of
our
analysis.
Furthermore,
the
study
population
we
chose
(children
aged
2–12
years)
is
younger
than
that
of
most
previous
studies,
making
comparisons
difficult.
| CONCLUSION
AND
RECOMMENDATIONS |
The
prevalence
of
overweight
and
obesity
among
children
is
increasing
in
the
UAE,
especially
among
UAE
nationals
and
in
late
childhood.
Most
parents
of
obese
children
fail
to
perceive
their
children
as
obese.
Parents
should
understand
the
huge
problem
of
obesity
and
its
impact
on
society.
Our
recommendation
is
to
focus
more
attention
on
UAE
nationals
and
children
during
early
childhood
by
means
of
a
robust
awareness
campaign
and
a
health
education
program
to
prevent
obesity.
In
addition,
schools
and
health
authorities
should
work
together
to
improve
the
sports
curriculum
and
find
a
solution
to
this
problem.
Acknowledgments
This
research
was
supported
by
the
Family
Medicine
Residency
Program
at
Sheikh
Khalifa
Medical
City.
We
thank
our
colleagues,
the
charge
nurses,
and
nurses
from
Bateen
and
Zafarana
clinic
who
helped
us
in
distributing
and
collecting
the
questionnaires.
We
would
also
like
to
show
our
gratitude
to
Dr.
Ebtihal
Darwish
for
sharing
her
experience
and
knowledge
that
greatly
assisted
the
research.
A
Al
Junaibi,
A.
A.-A.
(2012,
August).
The
prevalence
and
potential
determinants
of
§obesity
among
school
children
and
adolescents
in
Abu
Dhabi,
United
Arab
Emirates.
International
Journal
of
Obesity,
68–74.
A.A.
Bin
Zaal,
J.
B.
(2011).
Anthropometric
characteristics
and
obesity
among
adolescents
in
the
United
Arab
Emirates.
Eastern
Mediterranean
Health
Journal,
17,
382-386.
Abdulla
Aljunaibi,
A.
A.
(2013).
Parental
Weight
Perceptions:
A
Cause
for
Concern
in
the
Prevention
and
Management
of
Childhood
Obesity
in
the
United
Arab
Emirates.
Plos
One,
1-4.
Al-Haddad
FH,
A.-N.
Y.
(2000).
The
prevalence
of
obesity
among
school
children
in
the
United
Arab
Emirates:
Serious
public
health
implications.
J
Hum
Biol
12,
498–502.
Al-Haddad
FH,
L.
B.
(2005).
Childhood
obesity
in
United
Arab
Emirates
schoolchildren:
a
national
study.
Annals
of
Human
Biology,
72-79.
Al-Hourani
HM,
H.
C.
(2003).
Prevalence
of
overweight
among
adolescent
females
in
the
United
Arab
Emirates.
AMERICAN
JOURNAL
OF
HUMAN
BIOLOGY,
15,
758–764.
Blössner,
M.
d.
(2000).
Prevalence
and
trends
of
overweight
among
preschool
children
in
developing
countries.
American
Society
for
Clinical
Nutrition.
CDC.
(2015,
April
24).
Adolescent
and
School
Health:
Childhood
Obesity
Facts.
Retrieved
July
2,
2015,
from
Centers
for
Disease
Control
and
Prevention:
http://www.cdc.gov/healthyyouth/obesity/facts.htm
Cole
TJ,
B.
M.
(2000).
Establishing
a
standard
definition
for
child
overweight
and
obesity
worldwide
international
survey,
1-6.
Kelly
Stott,
T.
C.
(2012).
Teachers’,
Parents’
and
Children’s
Perceptions
of
Childhood
Obesity
in
Ras
Al
Khaimah.
Policy
Paper.
Malik,
M.
B.
(2007).
National
prevalence
of
overweight
and
obesity
among
children
in
the
United
Arab
Emirates.
Obesity
Reviews,.
Obesity
Reviews,
15-20.
T.
Lobstein,
L.
B.
(2004).
Obesity
in
children
and
young
people:
a
crisis
in
public
health.
The
International
Association
for
the
Study
of
Obesity.
obesity
reviews
5,
4-85.
Wagner,
C.,
&
Greer,
F.
(2008).
Prevention
of
Rickets
and
Vitamin
D
Deficiency
in
Infants,
Children,
and
Adolescents.
Journal
of
the
American
Academy
of
Pediatrics,
122
(5),
1142-1152.
WHO.
(2015).
dietphysicalactivity/childhood.
Retrieved
July
2,
2015,
from
http://www.who.int:
http://www.who.int/dietphysicalactivity/childhood/en/
|
|
.................................................................................................................

|
| |
|
